Home > Cancer Types > Head and Neck > Hypopharyngeal Cancer
Hypopharyngeal Cancer
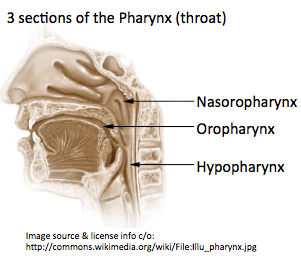 The hypopharynx is the bottom part of the pharynx (throat). The hypopharynx is sometimes also known as the laryngopharynx. Hypopharyngeal cancer occurs when the cells of the hypopharnx become abnormal and start growing in an uncontrolled way. The majority of hypopharyngeal cancers are squamous cell carcinomas (squamous cells are the thin, flat cells in the lining of the hypopharynx), but there are a number of other different types.
The hypopharynx is the bottom part of the pharynx (throat). The hypopharynx is sometimes also known as the laryngopharynx. Hypopharyngeal cancer occurs when the cells of the hypopharnx become abnormal and start growing in an uncontrolled way. The majority of hypopharyngeal cancers are squamous cell carcinomas (squamous cells are the thin, flat cells in the lining of the hypopharynx), but there are a number of other different types.
 Information for Patients and the Public Information for Health Professionals / Researchers Latest Research Publications
Information for Patients and the Public Information for Health Professionals / Researchers Latest Research PublicationsInformation Patients and the Public (6 links)
Information for Health Professionals / Researchers (5 links)
This list of publications is regularly updated (Source: PubMed).
Wong CK, Chan SC, Ng SH, et al.
Textural features on 18F-FDG PET/CT and dynamic contrast-enhanced MR imaging for predicting treatment response and survival of patients with hypopharyngeal carcinoma.Medicine (Baltimore). 2019; 98(33):e16608 [
PubMed]
Related Publications
The utility of multimodality molecular imaging for predicting treatment response and survival of patients with hypopharyngeal carcinoma remains unclear. Here, we sought to investigate whether the combination of different molecular imaging parameters may improve outcome prediction in this patient group.Patients with pathologically proven hypopharyngeal carcinoma scheduled to undergo chemoradiotherapy (CRT) were deemed eligible. Besides clinical data, parameters obtained from pretreatment 2-deoxy-2-[fluorine-18]fluoro-D-glucose positron emission tomography/computed tomography (F-FDG PET/CT), dynamic contrast-enhanced (DCE) magnetic resonance imaging (MRI), and diffusion-weighted MRI were analyzed in relation to treatment response, recurrence-free survival (RFS), and overall survival (OS).A total of 61 patients with advanced-stage disease were examined. After CRT, 36% of the patients did not achieve a complete response. Total lesion glycolysis (TLG) and texture feature entropy were found to predict treatment response. The transfer constant (K), TLG, and entropy were associated with RFS, whereas K, blood plasma volume (Vp), standardized uptake value (SUV), and entropy were predictors of OS. Different scoring systems based on the sum of PET- or MRI-derived prognosticators enabled patient stratification into distinct prognostic groups (P <.0001). The complete response rate of patients with a score of 2 was significantly lower than those of patients with a score 1 or 0 (14.7% vs 58.9% vs 75.7%, respectively, P = .007, respectively). The combination of PET- and DCE-MRI-derived independent risk factors allowed a better survival stratification than the TNM staging system (P <.0001 vs .691, respectively).Texture features on F-FDG PET/CT and DCE-MRI are clinically useful to predict treatment response and survival in patients with hypopharyngeal carcinoma. Their combined use in prognostic scoring systems may help these patients benefit from tailored treatment and obtain better oncological results.
- There are several options for hypopharyngeal reconstruction depending on defect size. Reconstructive options include primary closure, local flaps, regional axial flaps or regional intestinal flaps, and free flap transfer with skin or intestinal free flaps. The preferred method of reconstruction should minimize early postoperative complications that prolong hospital stay and/or become life threatening, ensure early restoration of function and decrease donor site morbidity. The purpose of this study was to evaluate functional outcomes of different flap reconstruction methods in type II hypopharyngeal defects. In this non-randomized retrospective cohort study, data on 31 (27 male and four female) patients were collected over a 10-year period of single institution type II hypopharyngeal defect reconstructions. The following measures of functional outcome were extracted from patient medical histories: postoperative complications (flap failure, fistula formation, donor site related complications), hospital stay in days and swallowing function after 14 days, 1 month and 6 months. There were nine patients in the radial forearm free flap (RFFF) reconstruction group, seven in the jejunum reconstruction group, and 15 in the gastric tube reconstruction group. In the RFFF group, three patients experienced flap failure; in the jejunal transfer group, no donor site morbidity was observed; whereas three patients from the gastric tube reconstruction group had minor abdominal skin wound dehiscence. Out of the 3 different reconstructive methods, RFFF was most likely to fail. The mean duration of hospital stay was 22.6 days, being shortest in the RFFF group. There were no significant differences in early postoperative swallowing function among the groups. The choice of flap used for hypopharynx reconstruction should be driven by donor site factors and functional outcomes. When assessing type II hypopharyngeal defect reconstruction results, the findings of this study suggest that free jejunal flaps and gastric tubes offer superior functional results in comparison with RFFFs.
This study used radiomics image analysis to examine the differences of texture feature values extracted from oropharyngeal and hypopharyngeal cancer positron emission tomography (PET) images on various tumor segmentations, and finds the proper and stable feature groups. A total of 80 oropharyngeal and hypopharyngeal cancer cases were retrospectively recruited. Radiomics method was applied to the PET image for the 80 oropharyngeal and hypopharyngeal cancer cases to extract texture features from various defined metabolic volumes. Kruskal-Wallis one-way analysis of variance method was used to test whether feature value difference exists between groups, which were grouped by stage, response to treatment, and recurrence. If there was a significant difference, the corresponding feature cutoff value was applied to the Kaplan-Meier estimator to estimate the survival functions. For the various defined metabolic volumes, there were 16 features that had significant differences between early (T1, T2) and late tumor stages (T3, T4). Five images and 2 textural features were found to be able to predict the tumor response and recurrence, respectively, with the areas under the receiver operating characteristic curves reaching 0.7. The histogram entropy was found to be a good predictor of overall survival (OS) and primary relapse-free survival (PRFS) of oropharyngeal and hypopharyngeal cancer patients. Textural features from PET images provide predictive and prognostic information in tumor staging, tumor response, recurrence, and have the potential to be a prognosticator for OS and PRFS in oropharyngeal and hypopharyngeal cancer.
Fagan JJ, Chaturvedi P, Kowalski LP
Treatment Options for Hypopharyngeal Cancer in Developing Countries in Africa/South America/Asia.Adv Otorhinolaryngol. 2019; 83:159-166 [
PubMed]
Related Publications
Most cancers occur in developing countries, and therefore, a discussion about cancer care would be incomplete without providing a developing world perspective. This chapter focuses on challenges and practices relating to hypopharyngeal cancer in limited-resource public healthcare systems in developing countries and specifically in Sub-Saharan Africa, India and South America and by extension, most patients in the developing world. Management of hypopharyngeal cancer must be adapted to the availability of specialised diagnostic and therapeutic services, radiotherapy and surgical expertise, and tailored to patient factors such as reliability of follow-up and social support. A particular challenge for physicians is to decide who can be denied the opportunity to be cured when the burden of cancer cases exceeds available resources. Public education campaigns about reducing risk factors for hypopharyngeal cancer are an important aspect of reducing the burden of cancer.
Siddiq S, Paleri V
Outcomes of Tumour Control from Primary Treatment of Hypopharyngeal Cancer.Adv Otorhinolaryngol. 2019; 83:90-108 [
PubMed]
Related Publications
Hypopharynx cancer continues to pose a clinically challenging head and neck subsite, driven not only by the unique set of patient, anatomic and disease factors but also by the paucity of robust clinical data to guide clinical decision making. The standard of care of radical surgery (pharyngolaryngectomy) in combination with postoperative radiotherapy was the previously accepted norm in the setting of advanced hypopharynx cancer, but this was often at the expense of significant morbidity. In the absence of survival benefit for advanced staged disease with radical surgical approaches, over the last 2 decades, the philosophy of quality of life in survivors has driven the agenda for new therapeutic approaches. The adoption of functional larynx preservation strategies has seen a paradigm shift in the treatment of this subsite since the 1990s with the advent of chemoradiation and intensity-modulated radiotherapy, thereby introducing a reducing trend for radical surgery. However, radical surgery (pharyngolaryngectomy) has a role in the non-functioning larynx (either pre- or post-treatment), in advanced volume disease and the more technically challenging salvage setting because of residual or recurrent disease. In earlier stage disease, transoral laser microsurgery and robotic surgery have shown good oncological benefits. Crucially, determining appropriate personalised treatment decisions in this challenging cohort of patients requires discussion within a multidisciplinary team framework.
Piazza C, Paderno A, Ravanelli M, Pessina C
Clinical and Radiological Evaluation of Hypopharyngeal Carcinoma.Adv Otorhinolaryngol. 2019; 83:35-46 [
PubMed]
Related Publications
Pre-treatment clinical and radiological evaluations represent a key step in the proper management of hypopharyngeal carcinoma. First, office-based endoscopy allows the assessment of superficial tumor extension, signs of laryngeal infiltration, and the overall residual function of the laryngo-hypopharyngeal complex. Different tools, maneuvers, and techniques can improve this essential diagnostic step and should be considered a prerequisite to direct subsequent investigations and give an initial indication for the most appropriate treatment. Furthermore, radiologic investigations help in determining tumor deep infiltration, lymph nodes involvement, and the presence of distant metastases. These should complement clinical evaluation by giving a more precise view of the disease characteristics, its overall behavior, and pattern of spreading. The aim of the current review is to summarize the key points that should be considered when approaching hypopharyngeal tumors from a diagnostic perspective, by presenting the main advantages and drawbacks of each technique.
Eckel HE, Bradley PJ
Treatment Options for Hypopharyngeal Cancer.Adv Otorhinolaryngol. 2019; 83:47-53 [
PubMed]
Related Publications
Patients with hypopharyngeal cancer are difficult to treat because they typically present with advanced disease, poor general health status and severe nutritional problems. Currently, treatment options for previously untreated and newly diagnosed hypopharyngeal cancer patients include surgery of the primary tumour and lymph nodes metastasis, radiotherapy, systemic medical treatment, including traditional chemotherapy and immunotherapy. Currently, a multimodal treatment approach is preferred using surgery, radiotherapy and systemic therapy with curative intent and best supportive care in patients considered unfit for curative treatment or patients presenting with distant metastatic spread. More detailed topics regarding the choice of treatment include biological and immunological host factors and their use for defining individualised cancer care, integration of novel therapies, integration of patient autonomy into clinical reasoning and dealing with patients' trade-offs between oncological outcome and individual quality of life, local availability of diagnostic therapeutic procedures and volume-outcome relationships for head and neck cancer surgery, radiotherapy and specialised supportive care. They also include considerations regarding potential delay between diagnosis and treatment, and between different treatment modalities within the frame of multimodal therapy. To date only one randomised trial comparing surgical versus non-surgical approaches has been published. Most randomised trials dealing with hypopharyngeal cancer compare different chemo- and radiotherapy regimen, but do not compare with a surgical approach. On the other hand, most studies on the results of surgery are best considered to be of low-quality case series. At the same time, many of the chemotherapy and radiation oncology studies in head and neck cancer include patients with different primary sites, where hypopharyngeal cancer patients when included usually account for a minority of the study population. Therefore, choosing the best treatment for an individual patient with hypopharyngeal cancer relies on personal experience and local expertise of the multidisciplinary team involved in the therapeutic process.
Bradley PJ
Symptoms and Signs, Staging and Co-Morbidity of Hypopharyngeal Cancer.Adv Otorhinolaryngol. 2019; 83:15-26 [
PubMed]
Related Publications
Early throat symptoms are common and a diagnosis of hypopharyngeal cancer rare; therefore, confirming or excluding a serious diagnosis is missed or overlooked by both the patient and the practitioner - however, symptoms such as throat clearing and food sticking, which persist in adult patients who have the social habit of tobacco usage and/or drink excessive alcohol should be examined by a specialist to exclude the presence of hypopharyngeal cancer. Late symptoms/signs include neck swelling (uni- or bilateral), dysphagia, odynophagia, otalgia, dysphonia, dyspnoea and stridor. Associated with advancing age and social habits, many patients have co-morbidities such as diabetes mellitus, respiratory, cardiovascular disease and behavioural health disorders that play a major role in selecting the optimal treatment and thus a likely worse long-term outcome. The majority of cases when diagnosed are at an advanced stage including evidence of local cervical nodal metastasis and distant metastasis. The TNM staging system continues to be the "gold standard" for reporting and evaluation of treatment outcomes, but more recent reports show that the use of "tumour volume" obtained from disease stage scanning of both the T and N stage are better predictors of a successful disease response outcome for the selection of a non-surgical option. Patients at presentation and those that survive curative treatment are associated with the highest risk of developing a second primary tu mour - synchronous or metachronous, involving the lung and/or the oesophagus.
Hypopharyngeal cancer is uncommon in the developed world; it is mostly diagnosed in men who smoke tobacco and consume excessive alcohol and uncommon in women. However, recent trends in the developed world show that there has been an annual increase in the percentage of women with hypopharyngeal cancer. In France, there has been a significant annual percentage change in the incidence of this form of cancer - a decrease in men and a greater increase in women since the 1980s. In the developing world, India, Taiwan and other countries, the incidence of hypopharyngeal cancer has increased in both men and women. These populations indulge widely in the social habit of tobacco usage at an earlier age, both smoking and chewing, excessive alcohol drinking, along with the chewing of the areca nut. Recent research has proven that areca nut alone is carcinogenic. The combination of tobacco and alcohol has a greater multiplicative impact on increasing the risk of cancer, while the involvement of areca nut remains to be proven. The World Health Organisation has commenced a Global Mission on the cessation of smoking and reduction of alcohol intake. The effect of this work has been credited with a reduction of hypopharyngeal and other head and neck cancers. While the younger aged should be the targeted population to avoid tobacco usage, the middle and older age of the population must be targeted for quitting smoking tobacco.
Bradley PJ, Füreder T, Eckel HE
Systemic Therapy, Palliation and Supportive Care of Patients with Hypopharyngeal Cancer.Adv Otorhinolaryngol. 2019; 83:148-158 [
PubMed]
Related Publications
Hypopharyngeal cancer patients have a very poor prognosis and limited therapeutic options. Seventy to eighty per cent of all hypopharyngeal cancer patients will require palliative and/or end-of-life care for incurable end-stage disease during the course of their illness. The overall proportion of hypopharyngeal cancer patients not qualifying for initial curative treatment, or requiring palliation and supportive care over time is higher than for any other subsite of the head and neck. Surgery and radiotherapy usually have a very limited role in this setting, while systemic therapy will usually compete with supportive care as the best approach. Advances in medicine and oncological treatments for the management of patients with recurrent head and neck cancer have given physicians the opportunity to prolong life where possible. However, this increase in survival might not be clinically meaningful if patients do not simultaneously experience palliative benefits, such as a reduction in symptoms and an improvement in their overall quality of life (QoL). The optimal outcome of palliative treatment is the control of symptoms with minimal treatment toxicities while improving QoL. It remains unclear if current palliative treatment options are better at improving QoL than the best supportive care. An intervention that results in insufficient or unacceptable functional status to the extent that the patient cannot achieve treatment goals - even in the course of prolonging life - is questionable. When used for palliative care purposes, surgery, chemotherapy and radiotherapy commonly have limited effectiveness in improving QoL. Moreover, if these treatments are not congruent with a patient's end-of-life goals, they could constitute low-value care.
Wei WI, Chan JYW
Surgical Treatment of Advanced Staged Hypopharyngeal Cancer.Adv Otorhinolaryngol. 2019; 83:66-75 [
PubMed]
Related Publications
It is not uncommon for patients with hypopharyngeal cancer to present at an advanced stage of disease. Surgical treatment provides a cure for the tumour with immediate relief from obstruction to the airway and the swallowing passage. Careful planning of surgery is important to ensure good outcome of treatment and prevent complications, some of which may be fatal. The shape of the hypopharynx resembles that of a funnel, with a wide circumference above in continuity with the oropharynx, and a small circumference below where it joins with the cervical oesophagus. As a result, while small tumours require the partial removal of the hypopharynx, large tumours, especially those involving the post-cricoid region, warrant a complete, circumferential pharyngectomy. For tumours that invade the cervical esophagus, transcervical approach is still feasible, and this is facilitated by the removal of the manubrium, allowing access to the tumour and resection with clear margins. In the presence of synchronous tumours lower down in the esophagus, pharyngo-laryngo-esophagectomy is indicated. Successful reconstruction of defects after tumour extirpation allows proper wound healing and early delivery of adjuvant radiotherapy. It is also important to ensure quick recovery of the long-term swallowing function. It ranges from the use of the soft tissue flap with skin island that is sutured as a patch to the remnants of the pharyngeal mucosa, to the use of a visceral flap, such as the free jejunal flap, to repair the circumferential pharyngectomy defects. The treatment protocol is personalized according to the extent of the tumour and the characteristics of the patients.
Eckel HE, Bradley PJ
Natural History of Treated and Untreated Hypopharyngeal Cancer.Adv Otorhinolaryngol. 2019; 83:27-34 [
PubMed]
Related Publications
Patients with hypopharyngeal cancers frequently present at advanced stage and in poor general health status. Their natural history is characterised by diffuse local primary disease, mucosal and submucosal spread, early cervical nodal metastasis, and a relatively high rate of distant spread. By the time of initial diagnosis, some 60% of all hypopharyngeal cancer patients will be with stage IV disease, some 5% will present with distant metastases, and almost 40% will have a significant reduction in performance status. Less than 20% are diagnosed with a localised early stage disease. A long-standing social habit of excess of alcohol and tobacco usage leads to cancerisation and accounts for the multiple, synchronous primary malignant lesions that occur in many hypopharyngeal cancer patients. The natural history of untreated head and neck squamous cell carcinoma has infrequently been documented in the medical literature. However, without understanding the natural history of hypopharyngeal cancer, patient counselling and clinical management are difficult. Less than 20% of untreated patients survive for > 12 months and only a small proportion of patients will survive for more than 2 years after initial diagnosis. The natural course of the disease in patients treated for cure or, at least, for the relief of symptoms, is certainly more favourable than that of those who are not suited for, or not willing to accept the adverse effects of treatment. However, treatment results are still considerably less encouraging than those that are being reported for other sub-sites of the head and neck region. Among all head and neck cancer sites, 5-year age-standardised relative survival is currently the poorest for cancer of the hypopharynx and the highest for larynx cancers, 25 and 59%, respectively. Among the head and neck cancers, only hypopharynx showed a low outcome (25% at 5 years), with survival figures ranging between ≤30 (North Ireland and Italy) and 8% (Bulgaria). Recent studies from the United States indicate that overall 5-year survival rates for hypopharyngeal cancer have improved significantly in recent years, with the average survival being ≥40%.
Meulemans J, Delaere P, Vander Poorten V
Primary Treatment of T1-T2 Hypopharyngeal Cancer: Changing Paradigms.Adv Otorhinolaryngol. 2019; 83:54-65 [
PubMed]
Related Publications
There has been a general shift in the treatment of hypopharyngeal cancer from open surgical techniques (either radical or partial "organ" preserving) toward non-surgi cal "organ preserving" strategies (radiotherapy [RT] or chemoradiotherapy [CRT]) and minimally invasive transoral laser microsurgery (TLM) or transoral robotic surgery (TORS). Oncologic outcomes reported are comparable whatever modality is chosen, but better functional outcomes are observed in the RT/CRT and TLM/TORS-treated patients. Because of the high rate of second primary malignancies, which influences overall survival, one could favor an up-front transoral surgical procedure as a primary treatment modality for early hypoharyngeal carcinoma, leaving the (chemo)radiotherapeutic option open for treatment of a likely later emerging second primary. However, the TLM and TORS studies report a high rate of adjuvant irradiation-based treatment for close or positive margin excisions. Concerning post-treatment functionality, both RT/CRT and TLM/TORS yield satisfactory results, especially when compared to the open surgical procedures, but it remains unclear which of these options will result in the long-term best laryngopharyngeal functional outcome. There is a need for multi-institutional randomized controlled trials comparing the long term oncologic and functional outcomes of up-front minimal invasive transoral surgery with/without adjuvant treatment, to a primary non-surgical organ preservation treatment.
Simo R, Rovira A, Townley W
Salvage Treatment Options after Failed Primary Treatment of Hypopharyngeal Cancer.Adv Otorhinolaryngol. 2019; 83:135-147 [
PubMed]
Related Publications
Recurrent hypopharyngeal cancer (rHPC) is a high-risk fatal disease associated with poor prognosis and high risk of complications in patients who are suitable to undergo salvage treatment. The treatment of such patients should be managed by a dedicated multidisciplinary team, most frequently a tertiary centre. and with the agreement of the patient. Close follow-up is crucial in achieving early detection and being able to treat the recurrence with curative intention. When persistent or recurrent disease is suspected, cross-sectional computed tomography imaging (CT) and positron emission tomography-CT scanning followed by panendoscopy with biopsies are the initial steps that need to be done in order to confirm diagnosis and accurate staging. The current treatment modality, which results in the best survival outcomes for rHCP is surgery. For most suitable patients, total pharyngolaryngectmy remains the best surgical modality, although open partial surgery OPS and transoral surgery are options for a small number of patients who have recurrences following treatment of an early stage disease. Free tissue transfer flaps or pedicled myocutaneous flaps will be necessary for most patients to reconstruct the excised pharynx. When making such a treatment plan it is most important to explain to each patient of the likely outcome both in terms of quantity and quality of life expectation. Many factors that are likely to increase the risk of treatment complications have been reported and are best anticipated and avoided. It is essential to perform a thorough preoperative assessment, follow a tried and trusted protocoled surgical plan and to have established enhanced recovery pathways for postoperative care that is available.
Eckel HE, Bradley PJ
Future Perspectives in Hypopharyngeal Cancer Care.Adv Otorhinolaryngol. 2019; 83:167-175 [
PubMed]
Related Publications
Recent advances in minimal access surgery have shown promise in the treatment of limited hypopharyngeal lesions. In spite of their functionally excellent results in individual patients, it currently remains unlikely that these approaches will gain a more major universal impact on hypopharyngeal cancer care. In advanced stage hypopharyngeal cancer, the use of the traditional radical surgery, such as laryngo-pharyngectomy, is no longer accepted by many patients. In recent years, most would rather opt for less mutilating treatment, preferring a non-surgical option. Patients, families and medical practitioners frequently ignore or misunderstand the associated mortality and morbidity consequence of such an approach. Although synergy between chemotherapy and radiotherapy enhances the efficacy of the treatment, chemo-radiation as currently used achieves a tumour response in < 80%, with relapses of the tumour during the follow-up period, indicating that surgery is the only effective treatment option as salvage. Advances in molecular research have improved our understanding of oncogenesis, tumour spread and the mechanisms of metastases. Innovative strategies have become available that manipulating tumours or the host to favour conditions receptive for disease eradication. These advances have gone through pre-clinical testing and are currently being used in early clinical trials using approaches such as replacement of defective genes, suicide gene therapy, and immunologic gene therapy. Precision oncology may eventually be able to predict which patients are more likely to respond to specific cancer therapies based on increasingly accurate, high-resolution biomarkers based on molecular diagnostics of individual tumours. Currently concentrating cancer treatment at specialised head and neck cancer institutions is likely to contribute faster and more sustained results at improving patient outcomes for hypopharyngeal cancer care than any individual innovation in surgery, radiation oncology or systemic treatment. Preventative work should continue by governments with the elimination of the preventable risk factors (abusive use of alcohol, tobacco and betel nut chewing) may reduce the incidence of the disease.
Mahalingam S, Spielmann P
Quality of Life Outcomes following Treatment of Hypopharyngeal Cancer.Adv Otorhinolaryngol. 2019; 83:126-134 [
PubMed]
Related Publications
Quality of life (QoL) is an important consideration in the management of individuals with head and neck cancer. The poor prognosis and significant impact of treatment modalities on function of the salivary glands, larynx and pharynx combine to make hypopharyngeal carcinoma a particularly challenging condition to treat. The impact of diagnosis and treatment on health related QoL is substantial. There is increased understanding that organ preservation does not necessarily correlate with function preservation as was previously expected. The impact on QoL, of chemoradiotherapy (CRT) or surgery, must be taken into account when managing individuals and deciding on treatment. Several QoL tools have been developed to understand the subjective consequences of functional impairment. The number and quality of studies specifically for hypopharyngeal carcinoma are low. The effects on QoL differ for surgery and CRT, as one would expect, but there are no demonstrable significant differences in most domains. Those treated with CRT show higher levels of dry mouth and sticky saliva, while those patients who have undergone surgery report greater levels of sensory disturbance. Significant differences were not noted in speech outcomes or global (general) health scores. The psychological morbidity and lack of good coping strategies are thought to play an important role in the high suicide rates of these patients (12-fold higher than the average population in the USA). Large, long-term, longitudinal studies of patients surviving treatment, answering both general and disease-specific questionnaires are required to direct clinicians towards the least morbid treatment strategies. The ability to cope and the availability of emotional support probably have a greater impact on subjective QoL than the functional outcomes of treatment.
Kotake K, Kai I, Iwanaga K, et al.
Effects of occupational status on social adjustment after laryngectomy in patients with laryngeal and hypopharyngeal cancer.Eur Arch Otorhinolaryngol. 2019; 276(5):1439-1446 [
PubMed]
Free Access to Full Article Related Publications
PURPOSE: This study was performed to examine the relationship of social adjustment with occupation and life changes in patients with laryngeal and hypopharyngeal cancer, from before laryngectomy to 1 year after hospital discharge.
METHODS: The subjects were 27 patients with laryngeal and hypopharyngeal cancer who were admitted to hospital for laryngectomy and provided informed consent for participation in the study. The patients answered questionnaire surveys before surgery, and 3, 6, and 12 months after hospital discharge. Regarding social adjustment, social functioning (SF) and mental health (MH) in SF-36V2 were used as dependent variables, and time, occupation status, age, family structure, and sex as independent variables. Repeated measures analysis of variance was used to examine the main effect, and second- and third-order interactions were also examined.
RESULTS: The age of the subjects was 62.9 ± 6.4 years and about 30% had an occupation. Loss of voice was the reason for 30% leaving work. In an examination of the main effects of the four variables, only age was significant regarding SF, and SF was favorable in subjects aged ≥ 64 years old. Regarding MH, age and family structure were significant, and MH was higher in older subjects who lived alone. The interaction between time and the other 3 variables was not significant. Only time/age/occupation was significant for MH. Regarding SF, a weak interaction was suggested, but it was not significant.
CONCLUSION: Older subjects showed better social adjustment, and those who lived alone had better MH. These findings may have been due to a reduced environmental influence. MH of subjects with an occupation decreased more at 3 months or later after hospital discharge, compared to those without an occupation. Especially for younger patients, development of new approaches is required to allow families and colleagues of patients to understand the difficulties of patients with laryngeal and hypopharyngeal cancer.
BACKGROUND: Hypopharyngeal and laryngeal neoplasms are both fatal and hard to catch in early stages. Yet which treatment is the most efficacious one still remain unanswered. This network meta-analysis (NMA) was conducted to investigate effectiveness of six therapies being utilized in clinical practice nowadays.
METHODS: PubMed and Embase were retrieved to synthesize data. Direct and indirect evidence was combined to compare efficacy of treatments. A relative ranking of the six regimens was calculated by the surface under the curve ranking area (SUCRA).
RESULTS: A total of 28 trials with 9109 patients were included in our NMA. Five endpoints investigated included 3/5-year overall survival (3/5-OS), 3/5-year disease free survival (3/5-DFS) and 5-year overall survival rate (5-OSR). In terms of all efficacy outcomes, radiotherapy combined with surgery (RT + S) proved to be better than other therapies while radiotherapy (RT) alone also performed well. Induction chemoradiotherapy (ICRT) was the best regarding 3-DFS (SUCRA = 0.846) while current chemoradiotherapy (CCRT) ranked first in 5-DFS (SUCRA = 0.933) according to SUCRA results. No significant differences were demonstrated in 5-DFS and 5-OSR as shown in the results of NMA.
CONCLUSIONS: RT combined with surgery turned out to be optimal therapy of all the outcomes while the efficacy of RT was relatively poorer in the treatment of patients with larynx stage III-IV and hypopharynx stage II-IV. Also, the good performance of CCRT and ICRT in terms of DFS made them as secondary recommended therapies. There is no significant difference between surgery and transoral laser microsurgery (TLM) alone.
Li Z, Shi X, Li H, et al.
Low expression of AIM2 combined with high expression of p‑STAT3 is associated with poor prognosis in hypopharyngeal squamous cell carcinoma.Oncol Rep. 2019; 41(4):2396-2408 [
PubMed]
Related Publications
Studies indicate that the AIM2 inflammasome plays an important role in tumor occurrence and development. The present study examined the prognostic significance of AIM2 expression and the correlation between AIM2 expression and p‑STAT3 expression in hypopharyngeal squamous cell carcinoma (HSCC), which remain unknown. AIM2 and p‑STAT3 were detected using immunohistochemistry (IHC) in 111 paraffin‑embedded tissue samples from primary HSCC sites and 20 samples from matched adjacent non‑malignant sites. Western blotting was utilized to investigate AIM2, p‑STAT3 and total STAT3 in 5 pairs of fresh tissue samples. Western blotting indicated that AIM2 expression was significantly lower (P<0.05), but that p‑STAT3 levels and the p‑STAT3/STAT3 ratio were higher (P<0.01) in HSCC tissues than in adjacent normal hypopharyngeal tissues. IHC analysis of the 111 HSCC samples revealed low AIM2 and high p‑STAT3 expression in 48 (43.2%) and 58 (52.3%) samples, respectively. High AIM2 expression and low p‑STAT3 expression were detected in 13 (75%) and 18 (90%) adjacent normal hypopharyngeal tissue samples, respectively. In the HSCC samples, low AIM2 expression was closely related to lymph node metastasis and intravascular tumor thrombus (P<0.05). Kaplan‑Meier survival curves revealed that low AIM2 levels were strongly associated with poor survival for HSCC patients (P<0.0001). Additionally, Cox proportional hazards regression models indicated that low AIM2 expression significantly predicted poor prognosis for HSCC patients (P<0.0001), and multivariate analysis revealed that AIM2 expression could be an independent prognostic factor for HSCC patients (P<0.0001). Furthermore, AIM2 expression was negatively correlated with p‑STAT3 expression in the HSCC tissue samples, and combined analysis revealed that patients with low AIM2 and high p‑STAT3 levels had the worst survival rate. Moreover, receiver operating characteristic (ROC) curve analysis confirmed that AIM2 was predictive of specific survival in all HSCC patients [area under the curve (AUC)=0.7160]. In conclusion, our data suggested that for HSCC patients, AIM2 and p‑STAT3 expression detected via IHC could serve as a biomarker to predict tumor progression and as an independent prognostic factor.
Tomioka T, Beppu T, Fujii T, et al.
Surgical management around the paratracheal area of hypopharyngeal cancer.Jpn J Clin Oncol. 2019; 49(5):452-457 [
PubMed]
Related Publications
OBJECTIVE: We aimed to clarify the suitable surgical management around the paratracheal area of patients who undergo total pharyngolaryngectomy based on the pathological results of hypopharyngeal cancer.
METHODS: The study was conducted under a multicenter, retrospective observational design in Japan. We analyzed histopathological paratracheal lymph node metastasis and thyroid invasion, and recurrence around the paratracheal area for 184 patients who underwent initial surgery among 280 participants.
RESULTS: There were significant differences in the frequency of metastasis to paratracheal lymph nodes as cN advances (P = 0.0344) and cT advances (P = 0.00028). By subsite, the paratracheal lymph node metastasis ratio was 22/130 patients (16.9%) in piriform sinus (PS), 8/32 (25.0%) in PW, 5/22 (22.7%) in PC and 10/17 (58.8%) in cervical esophagus (Ce+). The ratio of cases with bilateral paratracheal metastasis tended to be higher in cN2c, posterior wall (PW) and postcricoid (PC). Invasion to the thyroid was histopathologically confirmed in 16/184 patients (8.7%). Invasion from the primary lesion was in 15 patients.
CONCLUSION: This study indicates that it is better for patients with advanced hypopharyngeal cancer at minimum undergo ipsilateral paratracheal lymph node dissection. Tumor subsite of PW, PC or cN2c disease or disease extending to the Ce+ should be treated with bilateral paratracheal neck dissection. In order to more reliably perform paratracheal dissection, there is also an option to resect the thyroid lobe in the range of dissection. Preservation of the thyroid gland can be considered if invasion into the thyroid gland has been clearly ruled out.
PURPOSE: Although office-based transnasal esophagoscopy has been investigated extensively, a cost analysis is still lacking. We performed a cost analysis combined with feasibility study for two diagnostic processes: patients with globus pharyngeus and/or dysphagia, and hypopharyngeal carcinoma.
METHODS: Prospective cohort study.
RESULTS: Forty-one procedures were performed, of which 35 were fully completed. The procedure was well tolerated with mild complaints such as nasal or pharyngeal pain and burping. Four complications occurred: two minor epistaxis and two vasovagal reactions. In patients with globus pharyngeus and/or dysphagia, transnasal esophagoscopy resulted in a cost saving of €94.43 (p 0.026) per procedure, compared to our regular diagnostic process. In patients with suspicion of hypopharyngeal carcinoma, cost savings were €831.41 (p 0.000) per case.
CONCLUSIONS: Cost analysis showed that office-based transnasal esophagoscopy can provide significant cost savings for the current standard of care. Furthermore, this procedure resulted in good patient acceptability and few complications.
Akbaba S, Held T, Lang K, et al.
Salvage radiotherapy for recurrent hypopharyngeal and laryngeal squamous cell carcinoma (SCC) after first-line treatment with surgery alone: a 10-year single-centre experience.Radiat Oncol. 2019; 14(1):34 [
PubMed]
Free Access to Full Article Related Publications
PURPOSE: Salvage surgery of recurrent hypopharyngeal and laryngeal squamous cell carcinoma (SCC) results in limited local control and survival rates. As a result of recent technological progress, radiotherapy (RT) has become a valuable, potentially curative therapeutic option. Thus, we aimed to determine prognostic factors for survival outcome in order to optimize patient selection for salvage radiotherapy after failure of first-line treatment with surgery alone in this special patient cohort.
METHODS: Seventy-five patients (85% male, median age of 64 years) underwent salvage RT in a secondary setting for recurrent hypopharyngeal or laryngeal SCC after prior surgery alone between 2007 and 2017. On average, patients were treated with one prior surgery (range 1-4 surgeries). Median time between surgery and salvage RT was 7 months (range 1-47 months) for initially advanced tumors (T3/4, N+, extracapsular spread) and 18 months (range 5-333 months) for initially early stage tumors. The majority of patients received concomitant chemotherapy (n = 48; 64%) or other kind of systemic treatment concurrent to radiotherapy (n = 10; 13%).
RESULTS: Median follow-up was 41 months (range 3-120 months). Overall, fifteen patients were diagnosed with local failure (all were in-field) at last follow-up (20%). Median time to recurrence was 35 months (range 3-120 months) and 3-year local progression-free survival (LPFS) was 75%, respectively. Dose-escalated RT with 70.4 Gy applied in 2.1 Gy or 2.2 Gy fractions corresponding an EQD2 > 70 Gy (p = 0.032) and the use of concomitant cisplatin weekly chemotherapy (p = 0.006) had a significant positive impact on LPFS. 3-year OS and DPFS were 76 and 85%, respectively. No toxicity-related deaths occurred. Reported grade > 3 side effects were rare (n = 4/70, 6%).
CONCLUSION: Salvage radiotherapy resulted in excellent local control rates while radiation dose and the use of cisplatin weekly chemotherapy were identified as prognostic factors for LPFS. Nevertheless, patient selection for curative salvage treatment remains challenging.
Xu S, Yu Y, ElHakim H, et al.
The Therapeutic Effect of the Combination of Intratumor Injection of Bleomycin and Electroresection/Electrocautery on the Hemangiomas in Hypopharynx and Larynx Through Suspension Laryngoscopy.Ann Otol Rhinol Laryngol. 2019; 128(6):575-580 [
PubMed]
Related Publications
OBJECTIVES: The treatment of hemangiomas in the hypopharynx and larynx can be challenging and stressful because of the high tumor recurrence rate. The objective of this study was to investigate the therapeutic effect of the combination of intratumor injection of bleomycin and electroresection/electrocautery on the hemangiomas in the hypopharynx and larynx through suspension laryngoscopy.
METHODS: With patients under general anesthesia, the hemangiomas were fully exposed through suspension laryngoscopy. After intratumor injection of bleomycin, in some patients, the hemangiomas were completely resected along the bottom of the tumor pedicle by polypus-forceps electroscalpel; for other patients, the hemangiomas were pinched and held, and then the whole-tumor tissues were cauterized and coagulated by the electroscalpel. Prior to commencing the study, all participants signed informed consents, and all procedures were approved by the hospital ethical committee.
RESULTS: There was almost no bleeding during the operations, no postoperative dyspnea, and no hemorrhage. The patients were followed up for 3 years; the 3-year cure rate was 97%.
CONCLUSION: The hemangioma in the hypopharynx and larynx can be cured by a single-session treatment, using the combination of intratumor injection of bleomycin and electroresection/electrocautery through suspension laryngoscopy. Our method is reliable, affordable, and effective, and it could be widely applied in other hospitals.
The in vitro efficacy of cancer prodrugs varies significantly between malignant cell lines. The most commonly identified problems relate to delivery: uptake mechanism, endosomal entrapment, and drug release. Here we present the study of collagen/cell penetrating hybrid (COL/CPP) peptide carriers intended to deliver paclitaxel to the hypopharyngeal carcinoma (FaDu) cells. Confocal microscopy imaging revealed the surprising response of FaDu cell to COL/CPP in comparison to previously studied cancer cell lines: hybrid peptides that carry both COL and CPP domain adsorb on the FaDu cell surface. While the CPP domain was design to facilitate the cellular uptake, in the case of FaDu cells, it also induced detrimental interactions with the cell membrane. Despite surface adsorption, the colocalization study with endosomal markers EEA1 and LAMP1 reveals that COL/CPP is internalized via endosomal pathway, peptides are able to escape before lysosome formation and release paclitaxel. Therefore, the main obstacle for paclitaxel delivery to FaDu cells appears to be related to cell surface properties. This behavior seems specific to FaDu cells, and could be linked to previously reported overexpression of T5, heparanase splice variants that produces protein lacking enzymatic activity of heparanase. This results in increased concentration of HSPG on FaDu cell surface, and possibly creates a barrier for cellular uptake of highly charged COL/CPP.
Li L, Zou L, Fang J
A case report of application of posterior pharyngeal flap in resection and reconstruction of posterior pharyngeal wall carcinomas located at the level of the cricoid cartilage.Medicine (Baltimore). 2019; 98(7):e14412 [
PubMed]
Free Access to Full Article Related Publications
RATIONALE: posterior pharyngeal wall carcinomas located at the level of the cricoid cartilage is a rare occurrence. Surgical treatment is a dilemma owing to the retention of laryngeal function PATIENT CONCERNS:: A 56-year-old man underwent a "resection of left cervical tumor" at another hospital. Postoperative pathological report noted a left metastatic squamous cell carcinoma of the neck. Neck-enhanced computed tomography (CT) revealed thickening of the right posterior pharyngeal wall, and an image of soft tissue density was present on the posterior pharyngeal wall with a size of approximately 1.0 × 1.5 cm.
DIAGNOSIS: Hypopharyngeal carcinoma (T1N2M0).
INTERVENTIONS: We performed operation on a patient who suffered from posterior pharyngeal wall carcinomas at the level of the cricoid cartilage. The postoperative defects were repaired with posterior pharyngeal flaps.
OUTCOMES: The patient with posterior pharyngeal flap after operation survived without necrosis, the neck wounds of patient healed in 1 stage, and the phonation, swallowing and respiratory function was good.
LESSONS: The application of posterior pharyngeal flap to repair defects due to posterior pharyngeal wall carcinomas that were located at the level of the cricoid cartilage after resection is an effective reconstruction method that is easy to use and has excellent repair effects.
Eerenstein SEJ, Verdonck-de Leeuw IM, Leemans CR
Swallowing and Voice Outcomes following Treatment of Hypopharyngeal Cancer: The Need for Supervised Rehabilitation.Adv Otorhinolaryngol. 2019; 83:118-125 [
PubMed]
Related Publications
Advances in and intensification of treatment in hypopharyngeal cancer have led to an increase in organ preservation and in overall survival. Treatment intensification comes at the cost of more pronounced acute and long-term side effects causing functional impairments in voice and swallowing. Swallowing and voice problems have a significant impact on communication, eating and nutrition, social well-being and quality of life. Swallowing problems may be so severe that patients suffer profuse aspiration or are left gastrostomy-tube dependent. Pre-treatment evaluation of swallowing and voice as well as a tailored rehabilitation programme including personalized exercise prescriptions and advices on nutrition and weight, allows for a decrease and preferably prevention of the late effects. Although the evidence is still at a suboptimal level, there is general consensus to integrate prevention, monitoring and management of swallowing and voice impairments as part of treatment protocols. Optimal timing is still controversial, but a trend is seen to start voice and swallowing exercises prior to or at the start of treatment. However, patients are often reluctant to perform and adhere to the exercise prescriptions due to the burdensome tumour-treatment-schedules. This leads to a need for supervision, either face to face or online, during these rehabilitation programmes.
Sewnaik A, Baatenburg de Jong RJ
Sequelae and Complications of Treatment for Hypopharyngeal Cancer: Minimising the Risks.Adv Otorhinolaryngol. 2019; 83:109-117 [
PubMed]
Related Publications
Treatment of hypopharyngeal cancer depends on the extent and location of the tumour, patient-specific or by factors (age, performance status, co-morbidity) and the presence of psychosocial support. Options available for the treatment of hypopharyngeal cancer consist of surgery and non-surgery - radiotherapy, chemoradiation, bioradiation, or a combination of these modalities. To maintain normal functioning as much as possible, functional organ preservation is widely recommended and generally utilizes radiotherapy and/or chemoradiation. Although functional organ-sparing approaches can permit larynx preservation in patients with locoregionally advanced cancer of the hypopharynx, they do not provide a survival advantage over total laryngectomy. All available treatment modalities for patients with hypopharyngeal cancer have associated short- and long-term toxicities leading to side effects and complications.
de Bree R
The Current Indications for Non-Surgical Treatment of Hypopharyngeal Cancer.Adv Otorhinolaryngol. 2019; 83:76-89 [
PubMed]
Related Publications
The management of hypopharyngeal cancer is challenging because of poor patient survival and the potential effects of treatment on breathing, voice and swallowing. In general, early stage hypopharyngeal cancer can be primarily treated by radiotherapy or conservative transoral or open surgery, whereas advanced stage hypopharyngeal cancer can be treated by non-surgical protocols if the patient has no loss of functions (dysfunctional larynx) and/or cartilage invasion (T4a). Factors to determine individualized patient treatment include resectability, tumour volume, distant metastases, comorbidity, age, patient's preference, functional imaging parameters, response on induction chemotherapy and employing functional imaging parameters performed in the pre-treatment phase and repeated in the early treatment phase when employing a non-surgical treatment strategy.
Xu S, Hui L, Yang N, et al.
Upregulation of microRNA‑194‑5p inhibits hypopharyngeal carcinoma cell proliferation, migration and invasion by targeting SMURF1 via the mTOR signaling pathway.Int J Oncol. 2019; 54(4):1245-1255 [
PubMed]
Free Access to Full Article Related Publications
Hypopharyngeal carcinoma (HPC) is an aggressive malignancy with the worst prognosis among all head and neck cancers. MicroRNAs (miRNAs) are involved in the development of many human cancers, and may function as oncogenes or tumor suppressors. The present study aimed to evaluate the effects of miRNA (miR)‑194‑5p on the proliferation and invasion of HPC cells and to identify the potential regulatory mechanism. First, miR‑194‑5p and Smad ubiquitin regulatory factor 1 (SMURF1) expression levels were examined in HPC tissues. Subsequently, to explore the effects of miR‑194‑5p on SMURF1, a dual‑luciferase reporter gene assay was performed to verify the target relationship. To define the role of miR‑194‑5p in HPC progression, miR‑194‑5p upregulation and depletion were used to evaluate its effects on cell viability, invasion and migration. SMURF1 silencing and rapamycin [an inhibitor of the mammalian target of rapamycin (mTOR) signaling pathway] treatment were also used to analyze the regulatory mechanism in HPC. Finally, tumor growth was assessed in xenografted tumors in nude mice. SMURF1 was demonstrated to be highly expressed, whereas miR‑194‑5p was poorly expressed in HPC tissues; SMURF1 was identified as a target gene of miR‑194‑5p. FaDu hypopharyngeal squamous cell carcinoma cells treated with miR‑194‑5p mimics exhibited decreased viability, invasion and migration. The results indicated that miR‑194‑5p may inactivate the mTOR signaling pathway by targeting SMURF1. In addition, the in vivo experiments further verified these regulatory effects. These data suggested that miR‑194‑5p‑targeted SMURF1 inhibition may be involved in the disruption of HPC progression through the repression of the mTOR signaling pathway.
Li M, Xie M, Zhou L, Wang S
The impact of surgical margin status on the outcomes of locally advanced hypopharyngeal squamous cell carcinoma treated by primary surgery.Acta Otolaryngol. 2018; 138(12):1136-1145 [
PubMed]
Related Publications
BACKGROUND: The extent of surgical safety margin remained unclear in hypopharyngeal carcinoma surgery.
AIM: The purpose of this study was to evaluate the influence of surgical margin status on the outcomes of patients with advanced hypopharyngeal carcinoma.
MATERIAL AND METHODS: A retrospective analysis of clinical data was performed in 205 patients with stage III/IV hypopharyngeal carcinoma treated by primary surgery between January 2005 and December 2014. There were 129 patients with clear surgical margins (≥5 mm) and 76 with close surgical margins (<5 mm). The clinical characteristics and treatment outcomes were compared between the two groups.
RESULTS: Close surgical margin (cSM) was found to be a significant risk factor for local recurrence, overall survival (OS) and disease-specific survival (DSS). Analysis by stratification according to pT classification showed that the OS and DSS rates of T1/T2 tumors with clear surgical margins (nSM) were significantly higher than those with cSM (p < .05), while there was no significant difference in the OS and DSS rates between T3/T4 tumors with cSM and nSM (p > .05).
CONCLUSIONS AND SIGNIFICANCE: The tailored extent of surgical resection margin was recommended for locally advanced hypopharyngeal carcinomas according to primary tumor stage.
 Hypopharyngeal Cancer Treatment
Hypopharyngeal Cancer Treatment 
 US National Library of Medicine
US National Library of Medicine PubMed has over 22 million citations for biomedical literature from MEDLINE, life science journals, and online books. Constantly updated.
PubMed has over 22 million citations for biomedical literature from MEDLINE, life science journals, and online books. Constantly updated. Oropharyngeal Cancer
Oropharyngeal Cancer
