Oropharyngeal Cancer
 The oropharynx is the middle part of the pharynx (throat) behind the mouth. It is important for speach and swallowing. The oropharynx includes the soft palate, base of the tongue, side walls of the throat and the posterior pharyngeal wall. Oropharyngeal cancer occurs when the cells of the oropharynx become abnormal and start growing in an uncontrolled way. The majority of oropharyngeal cancers are squamous cell carcinomas (squamous cells are the thin, flat cells in the lining of the oropharynx), but there are a number of other different types.
The oropharynx is the middle part of the pharynx (throat) behind the mouth. It is important for speach and swallowing. The oropharynx includes the soft palate, base of the tongue, side walls of the throat and the posterior pharyngeal wall. Oropharyngeal cancer occurs when the cells of the oropharynx become abnormal and start growing in an uncontrolled way. The majority of oropharyngeal cancers are squamous cell carcinomas (squamous cells are the thin, flat cells in the lining of the oropharynx), but there are a number of other different types.
 Information for Patients and the Public Information for Health Professionals / Researchers Latest Research Publications
Information for Patients and the Public Information for Health Professionals / Researchers Latest Research PublicationsInformation Patients and the Public (8 links)
 Oropharyngeal Cancer Treatment
Oropharyngeal Cancer Treatment
National Cancer Institute![]() PDQ summaries are written and frequently updated by editorial boards of experts Further info.
PDQ summaries are written and frequently updated by editorial boards of experts Further info.
Cancer.Net![]() Content is peer reviewed and Cancer.Net has an Editorial Board of experts and advocates. Content is reviewed annually or as needed. Further info.
Content is peer reviewed and Cancer.Net has an Editorial Board of experts and advocates. Content is reviewed annually or as needed. Further info.
 Oropharyngeal cancer (cancer of the oropharynx)
Oropharyngeal cancer (cancer of the oropharynx)
Macmillan Cancer Support![]() Content is developed by a team of information development nurses and content editors, and reviewed by health professionals. Further info.
Content is developed by a team of information development nurses and content editors, and reviewed by health professionals. Further info.
Cancer Research UK
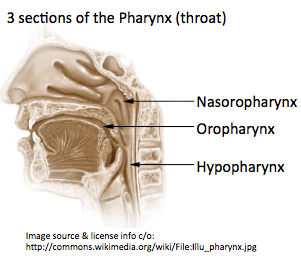
"Throat cancer is not a precise medical term...the medical name for the throat is the pharynx." The 3 main parts of the pharynx are the nasopharynx, oropharynx, and hypopharynx. However, some people sometimes use the term throat to include thyroid, larynx, esophagus, or trachia. Tracheal cancer is sometimes grouped with lung cancer.
Mouth and oropharyngeal cancer
Cancer Research UK
Oral Cavity and Oropharyngeal Cancer
Throat Cancer Foundation
Cleveland Clinic
Information for Health Professionals / Researchers (4 links)
- PubMed search for publications about Oropharyngeal Cancer - Limit search to: [Reviews]
PubMed Central search for free-access publications about Oropharyngeal Cancer
MeSH term: Oropharyngeal Neoplasms US National Library of Medicine
US National Library of Medicine PubMed has over 22 million citations for biomedical literature from MEDLINE, life science journals, and online books. Constantly updated.
PubMed has over 22 million citations for biomedical literature from MEDLINE, life science journals, and online books. Constantly updated.
Oropharyngeal Cancer Treatment
National Cancer Institute![]() PDQ summaries are written and frequently updated by editorial boards of experts Further info.
PDQ summaries are written and frequently updated by editorial boards of experts Further info.
Oropharyngeal and Hypopharyngeal Cancer Staging
Medscape
Article by Marvaretta Stevenson, MD.
SEER Stat Fact Sheets: Oral Cavity and Pharynx
SEER, National Cancer Institute
Overview and specific fact sheets on incidence and mortality, survival and stage,
lifetime risk, and prevalence.
Latest Research Publications
This list of publications is regularly updated (Source: PubMed).
Racial Disparities in Oropharyngeal Cancer Stage at Diagnosis.
Anticancer Res. 2017; 37(2):835-839 [PubMed] Related Publications
PATIENTS AND METHODS: The cohort included 18,791 adult patients diagnosed with oropharyngeal squamous cell carcinoma between 2004 and 2012, from the Surveillance, Epidemiology, and End Results 18 Database.
RESULTS: After adjusting for age, sex, marital status, tumor site, and year of diagnosis, black race was associated with increased risk of presenting with Stage III or IV disease (OR 1.24, p=0.016), T3 or T4 tumors (OR 2.16, <0.001), distant metastasis (OR 2, p<0.001), and unresectable tumors (OR 1.65, p<0.001). Race was not associated with risk of presenting with nodal metastasis diagnosis (OR 0.93, p=0.241).
CONCLUSION: Black race is associated with increased risk of advanced disease presentation in oropharyngeal cancer.
 USA
USA
Impact of Different Treatment Concepts on Regional Failure in Advanced Oropharyngeal Cancer.
Anticancer Res. 2017; 37(2):727-734 [PubMed] Related Publications
PATIENTS AND METHODS: Clinical data, including histological and radiological results, of 82 patients with T2-T3 oropharyngeal cancer and N2 neck were retrospectively analyzed. They underwent either RCT with salvage neck dissection (ND) (n=45), or primary transoral surgery with ND and adjuvant RCT (n=37). In all cases, the primary tumor was successfully treated, without evidence of local failure in the follow-up.
RESULTS: Overall, 11 (13.4%) patients developed regional failure during the follow-up. There were no significant differences in frequency of regional failure (p=0.75), distant metastasis (p=0.35) and overall survival (p=0.22) between treatment groups. However, 5-year disease-free survival was significantly worse (39.0% vs. 57.0%) for patients treated by RCT, with more frequent regional failure detected compared to surgically-treated patients in univariate analysis (p=0.04).
CONCLUSION: Treatment concept does not seem to affect regional tumor control in advanced oropharyngeal cancer after successful treatment of the primary tumor.
Multiple metastatic malignant phyllodes tumor of the breast with tonsillar metastasis: a case report.
BMC Res Notes. 2017; 10(1):55 [PubMed] Free Access to Full Article Related Publications
CASE PRESENTATION: A 57-year-old Japanese woman received surgery (partial mastectomy) of malignant phyllodes tumor. Seven months after initial surgery, pharyngeal pain, swelling, and a feeling of dyspnea developed, and tumor was found in the left palatine tonsil. Computed tomography for further evaluation showed a tonsillar lesion with contrast enhancement, and tonsillar metastasis was suspected. The metastatic lung tumors had not progressed. Laryngoscopic biopsy showed a tonsillar metastasis from the malignant phyllodes tumor. Despite the diagnosis of malignant phyllodes tumor with tonsillar and pulmonary metastases, the patient refused further treatment and died about 1 month later.
CONCLUSIONS: A patient with a malignant phyllodes tumor of the breast and tonsillar metastasis was reported, along with a discussion of the relevant literature of this very rare pattern of metastasis.
Breast Cancer
Minimally invasive surgery versus radiotherapy/chemoradiotherapy for small-volume primary oropharyngeal carcinoma.
Cochrane Database Syst Rev. 2016; 12:CD010963 [PubMed] Related Publications
OBJECTIVES: To assess the efficacy of endoscopic head and neck surgery (transoral robotic surgery or transoral laser microsurgery) for small-volume, primary (T1-2, N0-2) oropharyngeal squamous cell carcinoma (OPSCC) in comparison to radiotherapy/chemoradiotherapy.
SEARCH METHODS: The Cochrane ENT Information Specialist searched the ENT Trials Register; Central Register of Controlled Trials (CENTRAL 2016, Issue 10); PubMed; EMBASE; CINAHL; Web of Science; ClinicalTrials.gov; ICTRP and additional sources for published and unpublished trials. The date of the search was 8 November 2016.
SELECTION CRITERIA: Randomised controlled trials in patients with carcinoma in the oropharynx subsite (as defined by the World Health Organization classification C09, C10). Cancers included were primary squamous cell carcinomas arising from the oropharyngeal mucosa. The tumours were classified as T1-T2 with or without nodal disease and with no evidence of distant metastatic spread. The intervention was transoral, minimally invasive surgery with or without adjuvant radiotherapy or adjuvant chemoradiotherapy. The comparator was primary radiotherapy with or without induction or concurrent chemotherapy for the tumour. The treatments received and compared were of curative intent and patients had not undergone prior intervention, other than diagnostic biopsy.
DATA COLLECTION AND ANALYSIS: We used the standard methodological procedures expected by Cochrane. Our primary outcomes were overall survival (disease-related mortality was to be studied where possible), locoregional control, disease-free survival and progression-free survival or time to recurrence. All outcomes were to be measured at two, three and five years after diagnosis. Our secondary outcomes included quality of life, harms associated with treatment, patient satisfaction and xerostomia score.
MAIN RESULTS: No completed studies met the inclusion criteria for the review. Two ongoing trials fulfilled the selection criteria, however neither are complete.'Early-stage squamous cell carcinoma of the oropharynx: radiotherapy versus trans-oral robotic surgery (ORATOR)' is a phase II randomised controlled trial comparing primary radiation therapy with primary transoral robotic surgery for small-volume primary (T1-2, N0-2) OPSCC. It is currently in progress with an estimated completion date of June 2021.'European Organisation for Research and Treatment of Cancer 1420 (EORTC 1420-HNCG-ROG)' is a phase III, randomised study assessing the "best of" radiotherapy compared to transoral robotic surgery/transoral laser microsurgery in patients with T1-T2, N0 squamous cell carcinoma of the oropharynx and base of tongue. It was due to start accrual mid-2016.
AUTHORS' CONCLUSIONS: The role of endoscopic head and neck surgery in the management of OPSCC is clearly expanding as evidenced by its more overt incorporation into the current National Comprehensive Cancer Network guidelines. Data are mounting regarding its outcomes both in terms of survival and lower morbidity. As confidence increases, it is being used in the management of more advanced OPSCC.Based on this review, there is currently no high-quality evidence from randomised controlled trials regarding clinical outcomes for patients with oropharyngeal cancer receiving endoscopic head and neck surgery compared with primary chemoradiotherapy.
Impact of Induction Chemotherapy in Locally Advanced HPV-negative Oropharyngeal Cancer. A Propensity Score-matched analysis.
Anticancer Res. 2016; 36(12):6667-6672 [PubMed] Related Publications
PATIENTS AND METHODS: Consecutive patients with histologically-proven HPV-negative squamous cell carcinoma of the oropharynx were included and treated with IC-CRT or CRT alone. In order to compare treatment outcomes and toxicity between groups, patients were matched by primary tumor site and clinical disease stage. Overall survival (OS), disease-free survival (DFS) and metastasis-free survival (MFS) curves were calculated with the Kaplan-Meier method.
RESULTS: Nine IC patients and 18 CRT patients were included. All patients completed the programmed treatment. The median follow-up was 38 months. There were no statistically significant differences in OS and DFS between groups. The 5-year MFS was 88.9% and 50.8% in the IC-CRT group, respectively. There was no meaningful difference in toxicity between patients.
CONCLUSION: In HPV-negative patients with locally advanced oropharyngeal cancer, adding IC to standard CRT may increase the MFS rate. However no significant differences in OS and DFS were observed. More studies are needed to better elucidate the role of IC in this setting.
HPV-Positive Oropharyngeal Cancer Via p16 Immunohistochemistry in Japan.
Ann Otol Rhinol Laryngol. 2017; 126(2):152-158 [PubMed] Related Publications
METHODS: Fifty-nine oropharyngeal specimens from 2 university hospitals in Japan were examined for morphology and p16 immunohistochemistry. The rate of p16 positivity was then determined, and the 2 groups were compared for differences in age, smoking history, gender, and stage of presentation and mortality.
RESULTS: The rate of p16 positivity among the oropharyngeal specimens was 29.5%. There were important differences in the pathology compared to morphology usually seen in the US. The patients with p16+ cancer tended to be younger. There was no significant difference in smoking status. Patients with p16+ cancers trended toward better survival.
CONCLUSION: There appears to be a geographical difference in HPV rates of oropharyngeal cancers with persistently lower rates in Asian countries when compared to Western Europe and the US. Conclusions about HPV head and neck squamous cell carcinoma (HNSCC) in Western countries may not be generalizable across the globe at this time.
The Presence of HPV DNA in Neck Lymph Node Metastasis Correlates with Improved Overall Survival of Patients with Oropharyngeal Cancer Undergoing Surgical Treatment.
Oncology. 2017; 92(2):87-93 [PubMed] Related Publications
METHODS: A total of 65 patients who underwent surgery as a first-line therapy for OPSCC were enrolled in this study. In HPV-positive patients, the presence of HPV DNA in metastatic neck LN lesions was evaluated.
RESULTS: The HPV-positive patients had significantly better overall survival than the HPV-negative patients (log-rank test, p = 0.04), whereas HPV infection status did not significantly affect disease-free survival (log-rank test, p = 0.65). In all of the HPV-positive OPSCC patients who developed cervical LN metastasis, the same HPV DNA type was found in both the primary tumour and the metastases.
CONCLUSIONS: The present results suggest that HPV infection is a determining factor for good prognosis in patients undergoing first-line surgical therapy for OPSCC.
The changing landscape of oropharyngeal cancer management.
J Laryngol Otol. 2017; 131(1):3-7 [PubMed] Related Publications
METHOD: A literature review was conducted on the diagnosis and latest management of oropharyngeal cancer.
RESULTS: In non-smokers, human papilloma virus related disease is thought to have better outcomes, but this casts doubt on previous research which did not stratify patients according to human papilloma virus status. However, this theory provides a route for researchers to risk stratify and de-escalate treatments, and hence reduce treatment burden. In addition, the emergence of minimally invasive transoral techniques allows surgeons to remove large tumours without many of the side effects associated with radical (chemo)radiotherapy.
CONCLUSION: The emergence of human papilloma virus related disease and minimally invasive techniques have led the clinical and academic community to reconsider how oropharyngeal cancer is managed. Comparative and risk-stratification trials are urgently required and ongoing.
Oropharyngeal cancer: United Kingdom National Multidisciplinary Guidelines.
J Laryngol Otol. 2016; 130(S2):S90-S96 [PubMed] Free Access to Full Article Related Publications
Long-term survival outcomes in patients with surgically treated oropharyngeal cancer and defined human papilloma virus status.
J Laryngol Otol. 2016; 130(11):1048-1053 [PubMed] Related Publications
METHODS: A case note review was performed of all patients undergoing primary surgery for oropharyngeal cancer in a single centre over a 10-year period. Human papilloma virus status was determined via dual modality testing. Associations between clinicopathological variables and survival were identified using a log-rank test.
RESULTS: Of the 107 cases in the study, 40 per cent (n = 41) were human papilloma virus positive. The positive and negative predictive values of p16 immunohistochemistry for human papilloma virus status were 57 per cent and 100 per cent, respectively. At a mean follow up of 59.5 months, 5-year overall and disease-specific survival estimates were 78 per cent and 69 per cent, respectively. Human papilloma virus status (p = 0.014), smoking status (p = 0.021) and tumour stage (p = 0.03) were significant prognostic indicators.
CONCLUSION: The long-term survival rates in surgically treated oropharyngeal cancer patients were comparable to other studies. Variables including human papilloma virus status and tumour stage were associated with survival in patients treated with primary surgery; however, nodal stage and presence of extracapsular spread were non-prognostic.
Endovascular recanalization of the common carotid artery in a patient with radio induced chronic occlusion.
BMJ Case Rep. 2016; 2016 [PubMed] Related Publications
Exploring the Use of Oropharyngeal Cancer Histology to Account for HPV Status in Population-based Studies.
Anticancer Res. 2016; 36(10):5515-5518 [PubMed] Related Publications
PATIENTS AND METHODS: The study cohort included patients diagnosed with oropharyngeal squamous cell carcinoma between 2004 and 2012 identified in the Surveillance, Epidemiology, and End Results 18 Database.
RESULTS: Poorly differentiated tumors were associated with early T stage (odds ratio (OR)=1.23), nodal metastasis (OR=1.66) and tonsil fossa origin (OR=1.22). Non-keratinizing tumors were associated with early T stage (OR=1.23), nodal metastasis (OR=1.66) and tonsil fossa origin (OR=1.22). Poorly differentiated tumors were associated with improved overall survival (OS) (hazard ratio (HR)=0.78, p<0.001). Non-keratinizing tumors were associated with improved OS (HR=0.71, p<0.001).
CONCLUSION: Histological grade and keratinization may be useful surrogates to adjust for the effects of HPV status in oropharyngeal cancer studies utilizing population-based cancer databases.
Nivolumab-induced hypophysitis in a patient with advanced malignant melanoma.
Endocr J. 2016; 63(10):905-912 [PubMed] Related Publications
Monoclonal Antibodies Melanoma
Update on De-intensification and Intensification Studies in HPV.
Recent Results Cancer Res. 2017; 206:251-256 [PubMed] Related Publications
The Role of Surgery in the Management of Recurrent Oropharyngeal Cancer.
Recent Results Cancer Res. 2017; 206:197-205 [PubMed] Related Publications
The Role of Conventional Surgery in Oropharyngeal Cancer.
Recent Results Cancer Res. 2017; 206:185-195 [PubMed] Related Publications
Should We De-escalate the Treatment for HPV-Positive Tumors?
Recent Results Cancer Res. 2017; 206:173-181 [PubMed] Related Publications
Optimizing Radiotherapy in HPV-Associated Oropharyngeal Cancer Patients.
Recent Results Cancer Res. 2017; 206:161-171 [PubMed] Related Publications
Tumor Staging and HPV-Related Oropharyngeal Cancer.
Recent Results Cancer Res. 2017; 206:123-133 [PubMed] Related Publications
Risk Factors for Oral Infection with Human Papillomavirus.
Recent Results Cancer Res. 2017; 206:73-85 [PubMed] Related Publications
Selenium-binding protein 1 in head and neck cancer is low-expression and associates with the prognosis of nasopharyngeal carcinoma.
Medicine (Baltimore). 2016; 95(35):e4592 [PubMed] Free Access to Full Article Related Publications
METHODS: SELENBP1 gene expression in head and neck squamous cell carcinoma (HNSCC) was analyzed with GEO dataset and characteristics of SELENBP1 expression in paraffin embedded tissue were summarized. Expression of SELENBP1 in nasopharyngeal carcinoma (NPC), laryngeal cancer, oral cancer, tonsil cancer, hypopharyngeal cancer and normal tissues were detected using immunohistochemistry, at last, 99 NPC patients were followed up more than 5 years and were analyzed the prognostic significance of SELENBP1.
RESULTS: Analysis of GEO dataset concluded that SELENBP1 gene expression in HNSCC was lower than that in normal tissue (P < 0.01), but there was no significant difference of SELENBP1 gene expression in different T-stage and N-stage (P > 0.05). Analysis of pathological section concluded that SELENBP1 in the majority of HNSCC is low expression and in cancer nests is lower expression than surrounding normal tissue, even associated with the malignant degree of tumor. Further study indicated the low SELENBP1 expression group of patients with NPC accompanied by poor overall survival and has significantly different comparing with the high expression group.
CONCLUSION: SELENBP1 expression was down-regulated in HNSCC, but has no associated with T-stage and N-stage of tumor. Low expression of SELENBP1 in patients with NPC has poor over survival, so SELENBP1 could be a novel biomarker for predicting prognosis.
Primary surgery results in no survival benefit compared to primary radiation for oropharyngeal cancer patients stratified by high-risk human papilloma virus status.
Eur Arch Otorhinolaryngol. 2017; 274(1):477-487 [PubMed] Related Publications
Head and neck adaptive radiotherapy: Predicting the time to replan.
Asia Pac J Clin Oncol. 2016; 12(4):460-467 [PubMed] Related Publications
METHODS: Of 110 patients enrolled in a prospective H&N ART study, 21 (19%) underwent a second planning scan (re-CT) and were included in this review. Univariate and multivariate analysis was used to compare those patients who were replanned with those that were not. Factors influencing the timing of replanning were assessed including patient and tumor characteristics and structure volume details.
RESULTS: Of the five replanned patients, three were diagnosed with NPC (P = 0.06) and had significantly larger initial nodal volumes (median volume 140.3 cc vs. 39.1 cc, P = 0.019). Overall the median time of re-CT was significantly different between replanned and non-replanned patients, with replanned patients having an earlier re-CT: median fraction 18 versus fraction 23 (P = 0.01). Specifically, NPC patients who were replanned had a re-CT performed earlier than OPC patients (median fraction 11 vs. 20).
CONCLUSION: For H&N patients with large nodes receiving definitive chemoradiotherapy, replanning may be considered at the commencement of week 3 for NPC patients and in week 4 of treatment for OPC patients. This information may facilitate a forward planning approach to H&N ART that enables allocation of departmental resources prior to treatment commencement.
Nasopharyngeal Cancer
Oral sex and oropharyngeal cancer: The role of the primary care physicians.
Medicine (Baltimore). 2016; 95(28):e4228 [PubMed] Free Access to Full Article Related Publications
METHODS: We conduct a systemic review on the prevalence of oral sex among Americans among different age groups, the prevalence of HPV 16 infection reported in oropharyngeal cancer, and correlation between oral sex and oropharyngeal cancer.
RESULTS: Oral sex is prevalent among adolescents and sexually active adults. Sixty percent of oropharyngeal cancer reported in the United States is associated with HPV 16 infections. Individuals who practiced oral sex with multiple partners are at risk for developing oropharyngeal cancer and need to be informed about practicing safe sex or getting vaccination.
CONCLUSION: Family physicians will play a key role in prevention and educating the public about the risk of oral sex.
USA
Incidence of Oropharyngeal Cancer Among Elderly Patients in the United States.
JAMA Oncol. 2016; 2(12):1617-1623 [PubMed] Related Publications
Objective: To update the trends in OPSCC incidence using US cancer registry data, with an emphasis on age-specific trends.
Design, Setting, and Participants: Data from the Surveillance, Epidemiology, and End Results (SEER) database (2000-2012) were queried to compare changes in incidence and survival trends in OPSCC with selected tobacco-related cancers (larynx, oral cavity, hypopharynx, lung) and an HPV-related cancer (anus). A total of 40 264 patients who received a diagnosis of OPSCC from 2000 to 2012 were included. Elderly patients were defined as those 65 years or older.
Main Outcomes and Measures: The annual percentage change in OPSCC incidence from 2000 to 2012, stratified according to age group.
Results: Among the 40 264 patients who received a diagnosis of OPSCC from 2000 to 2012, 13 313 (33.1%) were aged 65 years or older and 80.3% were male. Significant increases in the age-adjusted incidence of OPSCC were observed during the study period for both younger adults aged 45 to 64 years (annual percentage change [APC], 2.31; 95% CI, 1.76-2.86; P < .001) and patients 65 years or older (APC, 2.92; 95% CI, 2.32-3.51; P < .001). These changes were driven predominantly by base-of-tongue and tonsil cancers in men. Concomitantly, the incidence of tobacco-associated head and neck cancers decreased for elderly patients (larynx: APC, -1.54; 95% CI, -2.00 to -1.08; P < .001; oral cavity: APC, -1.23; 95% CI, -1.84 to -0.62; P = .001; hypopharynx: APC, -2.44; 95% CI, -3.01 to -1.86; P < .001), whereas the incidence of anal cancer significantly increased (APC, 4.42; 95% CI, 3.28 to 5.57; P < .001). Furthermore, improved overall and cause-specific survival over time were observed for both younger and elderly patients with OPSCC. Nevertheless, absolute cause-specific survival remained worse for elderly patients (3-year CSS, 60.8%; 95% CI, 59.6%-61.9%) in comparison with those aged 45 to 64 years (75.7%; 95% CI, 75.1%-76.4%; P < .001).
Conclusions and Relevance: The incidence of OPSCC is increasing among elderly patients in the United States, likely driven by HPV-associated cancers. Given the unique challenges related to treating elderly patients with OPSCC, their limited enrollment in clinical trials, and the aging US population, clinical studies investigating improved therapeutic strategies for elderly patients with HPV-positive OPSCC should be performed.
USA
Adoption of transoral robotic surgery compared with other surgical modalities for treatment of oropharyngeal squamous cell carcinoma.
J Surg Oncol. 2016; 114(4):405-11 [PubMed] Free Access to Full Article Related Publications
METHODS: Cases of T1-T3 OPSCC treated with surgery between 2010 and 2013 from the National Cancer Database were queried.
RESULTS: Of 3,071 patients who underwent primary surgical management for T1-T3 OPSCC, 846 (28%) underwent TORS. On multivariable analysis, low tumor stage (T2 vs. T1: OR 0.75, CI 0.37-0.51, P < 0.0001; T3 vs. T1: O.R. 0.33, CI 0.28-0.38, P < 0.0001), treatment at an academic cancer center (O.R. 2.23, C.I. 1.29-3.88, P = 0.004) and treatment at a high volume hospital (34-155 cases vs. 1-4 cases: O.R. 9.07, C.I. 3.19-25.79, P < 0.0001) were associated with increased TORS approach. Significant geographic variation was observed, with high adoption in the Middle Atlantic. Positive margin rates were lower when TORS was performed at a high volume versus low volume hospital (8.2% vs. 16.7% respectively, P = 0.001).
CONCLUSIONS: Tumor and non-tumor factors are associated with TORS adoption. This analysis suggests uneven diffusion of this technology in the treatment of OPSCC. J. Surg. Oncol. 2016;114:405-411. © 2016 Wiley Periodicals, Inc.
Clinical features and treatment strategy for HPV-related oropharyngeal cancer.
Int J Clin Oncol. 2016; 21(5):827-835 [PubMed] Related Publications
Association between polymorphisms in genes related to DNA base-excision repair with risk and prognosis of oropharyngeal squamous cell carcinoma.
J Cancer Res Clin Oncol. 2016; 142(9):1917-26 [PubMed] Related Publications
METHODS: Aiming to identify the genotypes, DNA from 200 consecutive OPSCC patients and 200 controls was analyzed by PCR-RFLP. The prognostic impact of genotypes of SNPs on progression-free survival (PFS) and overall survival of OPSCC patients was examined using the Kaplan-Meier estimates and Cox regression analyses.
RESULTS: XRCC1 c.580CT or TT genotypes (19.5 vs. 11.0 %, P = 0.04) and XRCC1 TTGG haplotype from c.-77T>C, c.580C>T, c.839G>A and c.1196G>A SNPs (17.5 vs. 10.0 %, P = 0.04) were more common in patients with OPSCC than in controls. Carriers of combined genotypes of c.580C>T and TTGG haplotype of XRCC1 gene were under 3.35- and 3.22-fold increased risk of OPSCC than others. For survival analysis, we selected only patients with tumor at stage IV. The median follow-up time was 24.5 months. At 24 months of follow-up, PFS was shorter in patients with OGG1 c.977CC genotype when compared with others genotypes (35.5 vs. 52.1 %, log-rank test, P = 0.03). After multivariate Cox analysis, patients with OGG1 c.977CC genotype had more chance to present tumor progression when compared with others (HR 1.68, P = 0.02).
CONCLUSIONS: Our data present, for the first time, evidence that inherited OGG1 c.977C>G; XRCC1 c.-77T>C, c.580C>T, c.839G>A and c.1196G>A abnormalities of DNA BER pathway are important determinants of OPSCC and predictors of patient outcomes.
APEX1
Treatment: Outcome and Toxicity of Volumetric Modulated Arc Therapy in Oropharyngeal Carcinoma.
Anticancer Res. 2016; 36(7):3451-7 [PubMed] Related Publications
PATIENTS AND METHODS: Fifty-four patients presenting advanced orophayngeal carcinoma who were treated with radical radiotherapy were analyzed. All patients were treated with VMAT-RapidArc, with simultaneous integrated boost in 33 fractions for a dose of 69.96 Gy to the high-risk, and of 54.45 Gy to the low-risk volume.
RESULTS: Median follow-up was 23 months. In eight cases, locoregional relapse was observed (median time to relapse=10.7 months). Four among eight local recurrences appeared in the high-dose target volume. The 1- and 2-year actuarial disease-free survival rates were 88% and 80%, respectively. The 1- and 2-year actuarial overall survival rates were 94% and 87%, respectively.
CONCLUSION: VMAT for oropharyngeal SCC treatment is effective and safe, with interesting rates of control of disease and survival.
Survival and quality of life in oropharyngeal cancer patients treated with primary chemoradiation after salivary gland transfer.
J Laryngol Otol. 2016; 130(8):755-62 [PubMed] Related Publications
METHODS: A retrospective analysis of 138 patients (salivary gland transfer group, n = 58; non-salivary gland transfer group, n = 80) was performed. Patient survival was compared between these groups using multivariate analysis. Salivary gland transfer patients were further evaluated for surgical complications and for quality of life using the head and neck module of the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire.
RESULTS: Salivary gland transfer and non-salivary gland transfer patients had comparable baseline clinical characteristics. Salivary gland transfer patients experienced a median treatment delay of 16.5 days before chemoradiation (p = 0.035). Multivariate analysis showed that this did not, however, correspond to a survival disadvantage (p = 0.24 and p = 0.97 for disease-free and disease-specific survival, respectively). A very low complication rate was reported for the salivary gland transfer group (1.7 per cent). Questionnaire scores for the item 'xerostomia' were very low in salivary gland transfer patients.
CONCLUSION: The treatment delay associated with salivary gland transfer surgery does not negatively affect patient survival. Oropharyngeal squamous cell patients have an excellent quality of life after salivary gland transfer.
