Appendix Cancers
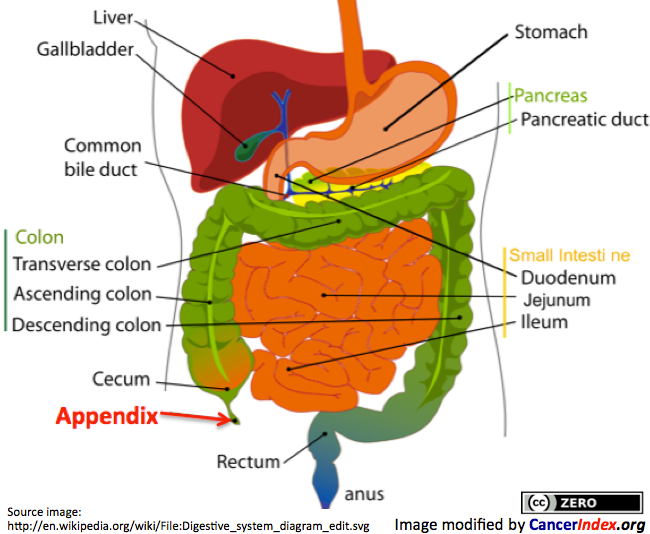 Cancer of the Appendix (also known as appendiceal cancer) occurs when cells in the appendix become abnormal and multiply without control. There are a range of different types of tumours and cancers which can start in the appendix. About two thirds of appendix tumours are carcinoid tumours which develop in hormone-producing cells that are present in many parts of the body, including the appendix. Mucinous cystadenocarcinoma account for about a fifth of appendix tumours, these produces mucin (a jelly-like substance). Pseudomyxoma Peritonei (PMP) is a more common name given to the "jelly belly" syndrome caused by mucinous adenoma and mucinous adenocarcinoma. Less common tumours of the appendix include signet-ring cell adenocarcinoma and paraganglioma. Treatment varies according to the type and stage of tumour.
Cancer of the Appendix (also known as appendiceal cancer) occurs when cells in the appendix become abnormal and multiply without control. There are a range of different types of tumours and cancers which can start in the appendix. About two thirds of appendix tumours are carcinoid tumours which develop in hormone-producing cells that are present in many parts of the body, including the appendix. Mucinous cystadenocarcinoma account for about a fifth of appendix tumours, these produces mucin (a jelly-like substance). Pseudomyxoma Peritonei (PMP) is a more common name given to the "jelly belly" syndrome caused by mucinous adenoma and mucinous adenocarcinoma. Less common tumours of the appendix include signet-ring cell adenocarcinoma and paraganglioma. Treatment varies according to the type and stage of tumour.
 Information for Patients and the Public Information for Health Professionals / Researchers Latest Research Publications
Information for Patients and the Public Information for Health Professionals / Researchers Latest Research Publications Gastrointestinal Carcinoid Tumours Gastrointestinal Cancers
Gastrointestinal Carcinoid Tumours Gastrointestinal CancersInformation Patients and the Public (13 links)
 Gastrointestinal Carcinoid Tumors Treatment
Gastrointestinal Carcinoid Tumors Treatment
National Cancer Institute![]() PDQ summaries are written and frequently updated by editorial boards of experts Further info.
PDQ summaries are written and frequently updated by editorial boards of experts Further info.
Cancer.Net![]() Content is peer reviewed and Cancer.Net has an Editorial Board of experts and advocates. Content is reviewed annually or as needed. Further info.
Content is peer reviewed and Cancer.Net has an Editorial Board of experts and advocates. Content is reviewed annually or as needed. Further info.

Cancer Research UK![]() CancerHelp information is examined by both expert and lay reviewers. Content is reviewed every 12 to 18 months. Further info.
CancerHelp information is examined by both expert and lay reviewers. Content is reviewed every 12 to 18 months. Further info.
Questions and asnwers
Macmillan Cancer Support![]() Content is developed by a team of information development nurses and content editors, and reviewed by health professionals. Further info.
Content is developed by a team of information development nurses and content editors, and reviewed by health professionals. Further info.
Appendiceal Cancer Advocacy Network
A patient-based advocacy organization, founded in 2004, dedicated to serving the needs of those diagnosed with cancer of the appendix.
Robert J. Miller, M.D - abourcancer.com
Short overview of appendix cancer and published abstract.
Founded by Carolyn Langlie-Lesnik RN BSN, a survivor of appendix cancer. The site includes information about the types of appendix cancer, treatment, survivors' stories, FAQ.
Promoting Awareness of PMP (Pseudomyxoma Peritonei), Appendiceal Cancer and other Peritoneal Surface Malignancies.
Support network and information about the various forms of appendix cancer.
A charitable organization founded in 2008 by a community of individuals affected by Pseudomyxoma Peritonei (PMP) and related Peritoneal Surface Malignancies (PSM). The site includes a FAQ and community information.
A registered charity which provides a support network for survivors and carers of Pseudomyxoma Peritonei. For those that are newly diagnosed, there is buddy system, Pseudomyxoma Buddies, which is free of charge and available UK wide.
Shooting for a Cure
Shooting for a Cure raises money for the Ric Summers Appendical Cancer Research Fund, linked to the MD Anderson Cancer Center in Houston.
Information for Health Professionals / Researchers (4 links)
- PubMed search for publications about Appendiceal cancer - Limit search to: [Reviews]
PubMed Central search for free-access publications about Appendiceal cancer
MeSH term: Appendiceal Neoplasms US National Library of Medicine
US National Library of Medicine PubMed has over 22 million citations for biomedical literature from MEDLINE, life science journals, and online books. Constantly updated.
PubMed has over 22 million citations for biomedical literature from MEDLINE, life science journals, and online books. Constantly updated.
Gastrointestinal Carcinoid Tumors Treatment
National Cancer Institute![]() PDQ summaries are written and frequently updated by editorial boards of experts Further info.
PDQ summaries are written and frequently updated by editorial boards of experts Further info.
Clinical Trials - Appendix carcinoma
National Cancer Institute
Latest Research Publications
This list of publications is regularly updated (Source: PubMed).
The Understated Malignancy Potential of Nonoperative Acute Appendicitis.
Am Surg. 2019; 85(7):712-716 [PubMed] Related Publications
 USA
USA
Risk of appendiceal cancer in patients undergoing appendectomy for appendicitis in the era of increasing nonoperative management.
J Surg Oncol. 2019; 120(3):452-459 [PubMed] Related Publications
MATERIALS AND METHODS: This retrospective cohort study was performed using the National Surgical Quality Improvement Program (NSQIP) appendectomy-targeted data set from 2016 to 2017. A total of 21 069 patients with imaging-confirmed or imaging indeterminate appendicitis who underwent appendectomy were included. Logistic regression was used to identify predictors of cancer diagnosis.
RESULTS: Increasing age had an increasing monotonic relationship with the odds of pathologic cancer diagnosis after appendectomy (age 50-59 odds ratio [OR], 2.08, 95% confidence interval [CI], 1.28-3.39, P = .003; age 60-69 OR, 2.89, 95% CI, 1.72-4.83, P < .001; age 70-79 OR, 3.85, 95% CI, 2.08-7.12, P < .001; age >80 OR, 5.32, 95% CI, 2.38-11.9, P < .001). Other significant predictors included obesity, morbid obesity, normal preoperative white blood cell count, and imaging indeterminate for appendicitis.
CONCLUSIONS: When counseling patients regarding operative vs nonoperative treatment options for management of acute appendicitis, the rising risk of a delayed or missed cancer diagnosis with increasing age must be discussed.
Systemic chemotherapy and survival in patients with metastatic low-grade appendiceal mucinous adenocarcinoma.
J Surg Oncol. 2019; 120(3):446-451 [PubMed] Article available free on PMC after 01/09/2020 Related Publications
METHODS: The National Cancer Database (2004-2015) was queried, and patients with mucinous, grade 1, stage IV appendiceal adenocarcinoma were identified. The Kaplan-Meier method was used to calculate survival, and a Cox regression model was used to identify predictors of survival.
RESULTS: Six hundred and thirty-nine patients were identified. Five-year overall survival (OS) for patients undergoing no chemotherapy vs chemotherapy was 52.9% and 61.3%, respectively. After adjusting with Cox proportional hazards model, chemotherapy was not associated with OS (HR:1.1, 95% CI:0.82-1.40, P = 0.61). Patients who underwent surgical resection (HR:0.40, 95% CI:0.28-0.57, P < .001) or were female (HR:0.61, 95% CI:0.5-0.8, P < .001) had improved survival in adjusted analysis.
CONCLUSIONS: There is no association between undergoing chemotherapy and OS in this cohort of patients with stage IV low-grade mucinous appendiceal adenocarcinoma. Development of national treatment guidelines is urgently needed for more consistency in the management of patients with appendiceal cancers.
USA
Rare causes of acute appendicitis.
Rozhl Chir. 2019; 98(5):189-193 [PubMed] Related Publications
METHODS: 1036 appendectomies were performed and 38 (3.7%) rare appendiceal tumor cases were identified at the department of Surgery in Pilsen from 1 January 2008 to 1 October 2018. The following text presents the difficult nature of the initial diagnosis, current therapy and principles of follow-up care in this relatively rare group of patients.
CONCLUSION: Appendiceal tumors are very rare. Depending on the histopathological type of tumor, it is necessary to choose adequate therapy and also provide proper follow up care.
Primary mixed adenocarcinoma and small-cell carcinoma of appendix: A case report (CARE-compliant).
Medicine (Baltimore). 2019; 98(19):e15614 [PubMed] Article available free on PMC after 01/09/2020 Related Publications
PATIENT'S CONCERN: A 70-year-old female was consulted to our Emergency Department with the right lower abdominal pain and low-grade fever for 2 days.
DIAGNOSIS: Abdominal ultrasonography revealed the perforated appendicitis with periappendiceal abscess. Postoperative histology confirmed the diagnosis of mixed SCC and adenocarcinoma.
INTERVENTIONS: After laparoscopic appendectomy, she underwent right hemicolectomy for radical surgery.
OUTCOMES: Laparoscopic appendectomy was performed and histological examination showed mixed SCC and adenocarcinoma. After confirming that there was no other organ metastasis, right hemicolectomy was performed for radical surgery. Five months after surgery, the patient expired due to multiple organ metastases.
LESSONS: Further studies are required for better understanding of disease entities, and clinical trials are needed to define adequate treatment strategies for extrapulmonary SCC.
Pseudomyxoma peritonei induced by low-grade appendiceal mucinous neoplasm accompanied by rectal cancer: a case report and literature review.
BMC Surg. 2019; 19(1):42 [PubMed] Article available free on PMC after 01/09/2020 Related Publications
CASE PRESENTATION: We present a unique case of a 70-year-old male with PMP induced by low-grade appendiceal mucinous neoplasm accompanied by rectal cancer. The patient's clinical, surgical, and histologic data were reviewed. The patient had persistent distended abdominal pain without radiating lower back pain, abdominal distension for 1 month, and no exhaustion or defecation for 4 days. A transabdominal ultrasound-guided biopsy was performed on the first day. The patient received an emergency exploratory laparotomy because of increased abdominal pressure. We performed cytoreductive surgery, enterolysis, intestinal decompression, special tumour treatment and radical resection of rectal carcinoma. The postoperative course was uneventful. The postoperative histological diagnoses were PMP, low-grade appendiceal mucinous neoplasm and rectal medium differentiated adenocarcinoma. At the 1-year follow-up visit, no tumour recurrence was observed by computed tomography (CT). We also performed a literature review.
CONCLUSIONS: We should be aware that PMP can rarely be accompanied by rectal cancer, which represents an easily missed diagnosis and increases the difficulty of diagnosis and treatment. Additionally, there are some typical characteristics of PMP with respect to diagnosis and treatment.
Anti-angiogenesis treatment in a patient with appendix metastasis of small cell lung cancer: A case report.
Medicine (Baltimore). 2019; 98(16):e15333 [PubMed] Article available free on PMC after 01/09/2020 Related Publications
PATIENT CONCERNS: We reported on a 52-year-old man who diagnosed as extensive stage SCLC with abdominal pain for 2 months, aggravated for 2 days.
DIAGNOSES: The patient was diagnosed with extensive-stage SCLC, relapsed with appendix metastasis after treatment by emergency abdominal surgery.
INTERVENTIONS: The patient received systemic treatments, including surgery, bevacizumab in combination with chemotherapy and bevacizumab alone was continued as maintenance therapy.
OUTCOMES: The patient had an overall survival would more than 23 months, and he gained another 8 months of progression-free survival after first-line radiochemotherapy.
LESSONS: Although SCLC appendix metastasis is rare, continuous anti-angiogenic therapy combined with bevacizumab maintenance therapy after surgical treatment can prolong survival.
Analysis of Treatment Failure after Complete Cytoreductive Surgery for Peritoneal Metastasis from Appendiceal Mucinous Neoplasm at a Japanese High Volume Center for Peritoneal Surface Malignancy.
Gan To Kagaku Ryoho. 2019; 46(2):251-258 [PubMed] Related Publications
METHODS: A total of 400 patients with AMCP who underwent complete cytoreductive surgery combined with perioperative chemotherapy were investigated.
RESULTS: Documented recurrence was developed in 135 (33.8%)patients. The 5- and 10-year progression-free survival was 51% and 49%, respectively. By multivariate analysis, histological subtype of peritoneal disease(high-grade AMCP[AMCP-H]and AMCP-H with signet ring cells), serum CA19- 9 level, and PCIB20 were significantly associated with reduced progression-free survival. In contrast, histologic subtype of mucin without epithelial cells(MWEC)showed the lowest risk for recurrence. Eighty-six patients had localized intra-abdominal recurrence, and 42 patients had diffuse peritoneal recurrence. Recurrence was found in the various peritoneal sectors. Eighty-one patients underwent complete cytoreduction for the recurrence, and the overall survival 5-year survival rate after secondary cytoreduction was 49%.
CONCLUSIONS: Risk factors for recurrence were histologic subtype, PCI cutoff level, and serum CA19-9 levels. Aggressive second attempt of cytoreduction in patients with localized recurrence improved the survival.
Neuroendocrine tumor of the appendix: Twelve years of results from a single institution.
Ulus Travma Acil Cerrahi Derg. 2019; 25(2):118-122 [PubMed] Related Publications
METHODS: Between February 2006 and June 2018, 6518 appendectomies were performed for acute appendicitis in the department of surgery, University of Health Sciences, Okmeydanı Education and Research Hospital, İstanbul, Turkey. The medical records of these consecutive 6518 appendectomy patients were evaluated retrospectively. After the histopathological analysis, a total of 22 patients were identified as cases of appendiceal NET. These patients were included in the study. A retrospective analysis of data including gender, age, intraoperative surgical findings, duration of postoperative follow-up and survival, tumor localization, the diameter of the tumor, tumor grade, invasion, surgical margin, and stage of the tumor was performed.
RESULTS: The incidence of appendiceal NET was 0.33%. Eleven patients were diagnosed as primary pathological stage pT1aN0M0 according to the European Neuroendocrine Tumor Society guidelines. One patient was diagnosed as primary pathological stage pT1bN0M0, and 10 patients were diagnosed as primary pathological stage pT2N0M0. The median tumor diameter was 7.6 mm. There was no patient with a tumor diameter greater than 20 mm.
CONCLUSION: The incidence of appendiceal NET in our study is consistent with that stated in the literature. The results of our research suggest that further surgical procedures for NETs that occur coincidentally in patients of the AA cohort are often unnecessary. In addition, the study revealed that disease-free survival (100%) was good over a mean follow-up of 59.2 months.
Long term survival analysis after hyperthermic intraperitoneal chemotherapy with oxaliplatin as a treatment for appendiceal peritoneal carcinomatosis.
Surg Oncol. 2019; 28:69-75 [PubMed] Related Publications
METHODS: Data was retrospectively reviewed and analyzed. Treatment consisted of CRS plus HIPEC with oxaliplatin. Ronnett's histologic classification was used (peritoneal mucinous carcinomatosis (PMCA), PMCA with intermediate features (PMCA-I) and disseminated peritoneal adenomucinosis (DPAM)). Overall survival (OS) and disease-free survival (DFS) estimates were calculated using Kaplan-Meier survival curves.
RESULTS: 109 patients with PC-A underwent laparotomy with curative intent. Of those, 92 underwent CRS plus HIPEC. Median follow-up was 42 months. The 5 and 10-year OS rates for the HIPEC group were 82.2% and 76.5%. The 5 and 10-year OS estimates for DPAM and PMCA-I subgroups were 100% and 100%, 78.1% and 72.9%, respectively. For the PMCA subgroup, the 3 and 5-year OS were 61.4% and 40.1%, respectively. The 5 and 10-year DFS estimates were 71.9% and 42.7%.
CONCLUSION: CRS plus HIPEC with oxaliplatin represent an effective therapeutic approach for PC-A. Long term OS estimates for patients treated at our institution are encouraging.
Oxaliplatin
Appendiceal Mass - Dilemmas Regarding Extension of the Resection.
Chirurgia (Bucur). 2019 Jan-Feb; 114(1):126-130 [PubMed] Related Publications
Appendiceal Malignancy: The Hidden Risks of Nonoperative Management for Acute Appendicitis.
Am Surg. 2019; 85(2):223-225 [PubMed] Related Publications
A unique presentation of superinfected pseudomyxoma peritonei secondary to a low-grade appendiceal mucinous neoplasm.
World J Surg Oncol. 2019; 17(1):34 [PubMed] Article available free on PMC after 01/09/2020 Related Publications
CASE PRESENTATION: A 46-year-old female with a past medical history notable for depression, asthma, and uterine leiomyomas presented to an urgent care with 5 days of progressive abdominal pain, bloating, nausea, and subjective fevers. The patient had a diffusely tender abdomen, without peritonitis, was mildly tachycardic, and had a white blood cell count of 15 K. A CT of the abdomen/pelvis was consistent with PMP with a ruptured appendiceal mucocele versus PMP secondary to an adnexal ovarian neoplastic pathology with an infectious component. The patient initially improved on antibiotics but ultimately required two surgeries, the first of which controlled intraabdominal sepsis while the second permitted definitive management of PMP with cytoreductive surgery (CRS) and HIPEC.
CONCLUSION: Superinfected PMP is a rare entity with very few documented cases. A staged approach that incorporates clearing the peritoneal infection, with or without resection of the primary tumor, followed by rehabilitation and definitive surgery appears to be a safe and effective management strategy.
Factors Predictive of Outcomes after Cytoreductive Surgery and Heated Intraperitoneal Chemotherapy for Colon and Appendiceal Carcinomatosis: A Single-Institution Experience.
Am Surg. 2018; 84(10):1575-1579 [PubMed] Related Publications
Leukocytoclastic vasculitis with late-onset Henoch-Schönlein purpura after trifluridine/tipiracil treatment.
Dermatol Online J. 2018; 24(10) [PubMed] Related Publications
Pleuropulmonary Recurrence Following Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemoperfusion for Appendiceal Pseudomyxoma Peritonei.
Ann Surg Oncol. 2019; 26(5):1429-1436 [PubMed] Related Publications
METHODS: From a prospective database, we identified patients who developed pleuropulmonary recurrence, isolated peritoneal recurrence, or no recurrence following CRS/HIPEC for appendiceal PMP. Clinicopathologic, perioperative, and oncologic data associated with the index CRS/HIPEC procedure were reviewed. The Kaplan-Meier method was used to estimate survival. Multivariate analyses identified associations with recurrence and survival.
RESULTS: Of 382 patients undergoing CRS/HIPEC, 61 (16%) developed pleuropulmonary recurrence. Patients who developed a pleuropulmonary recurrence were more likely to have high-grade (American Joint Committee on Cancer [AJCC] grade 2/3) tumors (74% vs. 56%, p = 0.02) and increased operative blood loss (1651 vs. 1201 ml, p = 0.05) and were more likely to have undergone diaphragm stripping/resection (79% vs. 48%, p < 0.01) compared with patients with an abdominal recurrence. In a multivariate analysis, pleuropulmonary recurrence after CRS/HIPEC was associated with diaphragm stripping/resection, incomplete cytoreduction, and higher AJCC tumor grade. There was a trend towards reduced survival in patients with pleuropulmonary recurrence compared with patients with isolated peritoneal recurrence (median overall survival 45 vs. 53 months, p = 0.87).
CONCLUSION: Pleuropulmonary recurrence of appendiceal PMP following CRS/HIPEC is common and may negatively impact survival. Formal protocols for surveillance and therapeutic intervention need to be studied and implemented to improve oncologic outcomes.
Lung Cancer
Review: Pathology and Its Clinical Relevance of Mucinous Appendiceal Neoplasms and Pseudomyxoma Peritonei.
Clin Colorectal Cancer. 2019; 18(1):1-7 [PubMed] Related Publications
Long term survival and perioperative propensity score matched outcomes in diaphragmatic interventions in cytoreductive surgery + intra-peritoneal chemotherapy.
Eur J Surg Oncol. 2019; 45(4):620-624 [PubMed] Related Publications
METHODS: 1230 consecutive CRS/IPC procedures were preformed between 1996 and 2018 in Sydney, Australia. Redo procedures and incomplete cyto-reductions were excluded. Among these, 599 underwent diaphragmatic intervention. Preoperative heterogeneity was assessed for in 6 parameters and addressed with propensity score matching. CRS/IPC requiring diaphragmatic interventions were compared to CRS/IPC without diaphragmatic involvement. Ten perioperative outcomes were measured. Overall survival was assessed based on diagnosis type.
RESULTS: Intraoperative results revealed a significant increase in operative hours (7.85 vs. 7.28, p = 0.033). Transfusion requirements were insignificantly different. Postoperatively, increased grade III and IV complications (36% vs. 26%, p = 0.052) were noted. There was no difference with regards to intensive care stay, hospital length of stay, hospital death and return to theatre. In terms of respiratory specific complications, an increased incidence of pneumothorax (13% vs. 3%, p = 0.001) and pleural effusions (24% vs. 16%, p = 0.043) were noted, whilst the differences in pneumonia were insignificant. Overall survival revealed diaphragm interventions; did not affect survival outcomes in colorectal cancers (p = 0.750, RR = 1.077, CI 0.683-1.697) and increased relative risk in low-grade appendiceal mucinous neoplasms (p = 0.025, RR = 2.437, CI 1.121-5.298).
CONCLUSION: After our three-tiered research strategy, we conclude that despite the marginal increase in short term morbidity; diaphragmatic interventions do not decrease survival in colorectal cancers and diaphragmatic disease in LAMNs maybe an independent prognosticator of disease aggression.
Introducing the eighth edition of the tumor-node-metastasis classification as relevant to colorectal cancer, anal cancer and appendiceal cancer: a comparison study with the seventh edition of the tumor-node-metastasis and the Japanese Classification of Colorectal, Appendiceal, and Anal Carcinoma.
Jpn J Clin Oncol. 2019; 49(4):321-328 [PubMed] Related Publications
METHODS: The eight edition was compared with the seventh edition as well as the Japanese Classification of Colorcetal, Appendiceal, and Anal carcinoma ninth edition.
RESULTS: Of colon and rectum, the tumor-node-metastasis eighth edition expands the M category. Specifically, colorectal cancer with peritoneal metastasis is newly categorized as M1c, distinguishing it from M1a (metastasis to one organ) and M1b (metastasis to more than one organ). In the ninth edition of Japanese Classification of Colorectal, Appendiceal, and Anal Carcinoma, M1c is further subdivided into M1c1 (metastasis to the peritoneum without other organ involvement) and M1c2 (metastasis to the peritoneum with other organ involvement). In the T category, the tumor-node-metastasis eighth edition excludes high-grade dysplasia (intraepithelial carcinoma) from Tis; this differs from both the tumor-node-metastasis seventh edition and the Japanese Classification of Colorectal, Appendiceal, and Anal Carcinoma ninth edition. In the N category, the tumor-node-metastasis eighth edition does not add the number of tumor deposits to the number of positive regional lymph nodes, whereas this number is added in the Japanese Classification of Colorectal, Appendiceal, and Anal Carcinoma ninth edition. The definition of anal cancer is also modified considerably in the tumor-node-metastasis eighth edition; specifically, tumors of perianal skin defined as within 5 cm of the anal margin are also classified as anal canal carcinoma, external iliac lymph nodes become regional lymph nodes, and both N2 and N3 are abolished in the N category. With regard to appendix, Tis (low-grade appendiceal mucinous neoplasma) and tumor deposit(s) are newly introduced. Finally, the tumor-node-metastasis eighth edition offers a new structure, labeled a 'prognostic factors grid', which consists of prognostic factors for survival in both colorectal and anal cancer.
CONCLUSIONS: Staging classification is updated regularly, which clinicians should always catch up with.
Anal Cancer
Goblet Cell Carcinoid/Carcinoma: An Update.
Adv Anat Pathol. 2019; 26(2):75-83 [PubMed] Related Publications
Outcomes in Peritoneal Dissemination from Signet Ring Cell Carcinoma of the Appendix Treated with Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy.
Ann Surg Oncol. 2019; 26(2):473-481 [PubMed] Related Publications
METHODS: A prospective database of CRS/HIPEC procedures for HGMCP performed from 1998-2017 was reviewed. Perioperative variables and survival were analyzed.
RESULTS: Eighty-six HGMCP and 65 HGMCP-S were identified. HGMCP had more positive tumor markers (TM) (CEA/CA-125/CA-19-9) than HGMCP-S (63% vs 40%, p = 0.005). HGMCP had higher Peritoneal Cancer Index (32 vs 26, p = 0.097) and was less likely to have positive lymph nodes (LN) than HGMCP-S (28% vs 69%, p = < 0.001). Complete cytoreduction was achieved in 84% and 83%, respectively. PFS at 3- and 5-years was 59% and 48% for HGMCP vs 31% and 14% for HGMCP-S. Median PFS was 4.3 and 1.6 years, respectively (p < 0.001). OS at 3- and 5-years was 84% and 64% in HGMCP vs 38% and 25% in HGMCP-S. Median OS was 7.5 and 2.2 years, respectively (p < 0.001). LN negative HGMCP-S had longer median PFS and OS than LN positive HGMCP-S (PFS: 3.4 vs 1.5 years, p = 0.03; OS: 5.6 vs 2.1 months, p = 0.021).
CONCLUSIONS: The aggressive histology of HGMCP-S is associated with poor OS, has fewer abnormal TM, and is more likely to have positive LN. However, CRS/HIPEC can achieve a 5-year survival of 25%, which may improve to 51% with negative LN.
Sites of Recurrence After Complete Cytoreduction and Hyperthermic Intraperitoneal Chemotherapy for Patients with Peritoneal Carcinomatosis from Colorectal and Appendiceal Adenocarcinoma: A Tertiary Center Experience.
Ann Surg Oncol. 2019; 26(2):482-489 [PubMed] Related Publications
METHODS: Patients undergoing optimal CRS/HIPEC (2007-2016) at the authors' institution were retrospectively reviewed from a prospectively maintained database. Data regarding disease recurrence were analyzed.
RESULTS: Of 74 patients who underwent CRS/HIPEC for PC from CRC (n = 46) or AC (n = 28), 49 (66%) had recurrence during a median follow-up period of 39.5 months. The sites of recurrence were peritoneal-only (n = 34, 69%), hematogenous-only (n = 6, 12%), and combined peritoneal and hematogenous (n = 9, 19%) sites. No patients with AC had hematogenous-only recurrence. The median disease-free survival (DFS) time for all the patients was 15 months (95% confidence interval [CI] 12.5-17.5 months). The recurrence rate after CRS/HIPEC was 41% at 1 year, 73% at 3 years, and 76% at 5 years. All the patients with hematogenous-only metastases experienced recurrence within 12 months after CRS/HIPEC. Mucinous or signet ring features predicted peritoneal recurrence (p = 0.041), whereas a complete cytoreduction of 1 was a predictor of early recurrence (p = 0.040). Patients who underwent repeat cytoreduction survived longer than those who received systemic chemotherapy alone. The median survival time after peritoneal-only recurrence was 33 months (95% CI 27.8-38.9 months).
CONCLUSION: Recurrence for patients with PC is common, even after optimal CRS/HIPEC. Hematogenous-only recurrence occurs early after CRS/HIPEC, suggesting occult disease at the time of treatment and highlighting the need for methods to identify micro-metastases and improve patient selection. Patients experiencing peritoneal-only recurrence had long survival period after CRS/HIPEC, suggesting its effectiveness at controlling peritoneal disease for a time.
Colorectal (Bowel) Cancer
Clinicopathological characteristics and prognosis of primary appendiceal stromal tumors.
World J Surg Oncol. 2018; 16(1):225 [PubMed] Article available free on PMC after 01/09/2020 Related Publications
METHODS: The PASTs described in this study were identified from a literature review (23 cases) and our center (one case). The relationship between PAST gross types and clinicopathological factors was analyzed and summarized. At the same time, the study also analyzed the related risk factors and survival of PASTs and GISTs.
RESULTS: Twenty-four cases of PASTs were compared with 254 cases of GISTs from our center. The results showed that there was a significant difference between the two groups in tumor size (P < 0.001), histological type (P = 0.013), CD34 expression (P < 0.001), and DOG-1 expression (P < 0.001). Disease-free survival (DFS) analysis of 11 cases of PASTs and 227 cases of GISTs found that a comparison of 3-year and 5-year DFS was not statistically significant (P = 0.894 and P = 0.846, respectively). In the DFS multivariate analysis, tumor mucosal ulceration, tumor size, and NIH risk classification were independent prognostic factors in 3-year and 5-year DFS.
CONCLUSION: In this study, there was no significance in the survival of patients with appendix and gastric stromal tumors, which we hypothesized to be associated with the low sample size and incomplete follow-up records. Based on this, we conclude that the prognosis of primary appendiceal stromal tumors may be better than gastric tumors, but this needs to be confirmed in further prospective studies.
Outcomes of Low-Grade Appendiceal Mucinous Neoplasms with Remote Acellular Mucinous Peritoneal Deposits.
Ann Surg Oncol. 2019; 26(1):118-124 [PubMed] Article available free on PMC after 01/01/2020 Related Publications
OBJECTIVE: This study was aimed at evaluating the relevance of mucin cellularity for predicting outcomes of LAMN with remote MPD.
METHODS: The records of patients with LAMN and remote MPD who underwent initial assessment at a comprehensive cancer center from 1990 to 2015 were reviewed, and diagnostic procedures, treatments, and outcomes were analyzed.
RESULTS: Of 48 patients included in the analysis, 19 had cellular MPD (CMPD) and 29 had acellular MPD. Of 33 patients who underwent cytoreductive surgery, 30 had a complete cytoreduction; the 3 patients with an incomplete cytoreduction had CMPD. In the follow-up period (median, 4 years), 6 patients died of the disease, all of whom had CMPD. Of 11 patients who had progression of disease, 10 had CMPD.
CONCLUSION: Cellularity of remote MPD is an important determinant of disease outcome in LAMN. Approaches such as active surveillance may have a role in selected patients with LAMN and AMPD.
Appendiceal Cancer Patient-Specific Tumor Organoid Model for Predicting Chemotherapy Efficacy Prior to Initiation of Treatment: A Feasibility Study.
Ann Surg Oncol. 2019; 26(1):139-147 [PubMed] Related Publications
METHODS: Appendiceal cancer specimens obtained during cytoreduction with hyperthermic intraperitoneal chemotherapy procedures (CRS/HIPEC) were dissociated and incorporated into an extracellular matrix-based hydrogel system as three-dimensional (3D), patient-specific tumor organoids. Cells were not sorted, preserving tumor heterogeneity, including stroma and immune cell components. Following establishment of organoid sets, chemotherapy drugs were screened in parallel. Live/dead staining and quantitative metabolism assays recorded which chemotherapies were most effective in killing cancer cells for a specific patient. Maintenance of cancer phenotypes were confirmed by using immunohistochemistry.
RESULTS: Biospecimens from 12 patients were applied for organoid development between November 2016 and May 2018. Successful establishment rate of viable organoid sets was 75% (9/12). Average time from organoid development to chemotherapy testing was 7 days. These tumors included three high-grade appendiceal (HGA) and nine low-grade appendiceal (LGA) primaries obtained from sites of peritoneal metastasis. All tumor organoids were tested with chemotherapeutic agents exhibited responses that were either similar to the patient response or within the variability of the expected clinical response. More specifically, HGA tumor organoids derived from different patients demonstrated variable chemotherapy tumor-killing responses, whereas LGA organoids tested with the same regimens showed no response to chemotherapy. One LGA set of organoids was immune-enhanced with cells from a patient-matched lymph node to demonstrate feasibility of a symbiotic 3D reconstruction of a patient matched tumor and immune system component.
CONCLUSIONS: Development of 3D appendiceal tumor organoids is feasible even in low cellularity LGA tumors, allowing for individual patient tumors to remain viable for research and personalized drug screening.
Postoperative Complications Independently Predict Cancer-Related Survival in Peritoneal Malignancies.
Ann Surg Oncol. 2018; 25(13):3950-3959 [PubMed] Related Publications
METHODS: The study used a prospective database of 1296 patients with peritoneal metastases (PM) undergoing CRS-HIPEC between 2001 and 2016. The Kaplan-Meier method was used to estimate survival. Multivariate analyses identified associations with perioperative and oncologic outcomes. The Akaike information criterion and the Schwarz (Bayesian information) criterion were used to compare model fitting for CCI versus CDC.
RESULTS: In this study, CRS-HIPEC was performed for malignant mesothelioma (12%) and PM from appendix (50%), colorectal (30%), and ovarian (8%) cancers. Major postoperative in-hospital complications (CDC grades 3-4) occurred for 24% of the patients. However, a range of CCI scores was calculated for each CDC grade because 36% of the patients experienced multiple complications. After a median follow-up period of 55 months, the median progression-free survival was 15 months, and the median overall survival was 39 months. In the multivariate Cox proportional hazards models, postoperative in-hospital complications (measured by CDC or CCI) were independent prognostic factors for 30-day post-discharge morbidity and readmission, as well as for survival. The CCI scores demonstrated higher prognostic sensitivity for these outcomes than CDC grades.
CONCLUSIONS: Reduction of postoperative complications after CRS-HIPEC is essential for optimal short- and long-term outcomes. For assessing total burden of postoperative complications per patient, CCI is superior to CDC and more sensitive for assessing surgery- and cancer-related outcomes after CRS-HIPEC.
Long-term Survival and Propensity Score Matched Outcomes of Bilateral
Anticancer Res. 2018; 38(10):5917-5921 [PubMed] Related Publications
PATIENTS AND METHODS: A total of 652 CRS/IPC procedures, between 1996 and 2018, required diaphragm interventions. Among these, 388 underwent bilateral intervention. Preoperative heterogeneity was assessed in 6 parameters and addressed with propensity score matching. The association of each respective analysis was assessed with 11 outcomes. Overall survival was assessed based on histology.
RESULTS: CRS/IPC requiring bilateral diaphragmatic interventions illustrated significantly increased operative hours (9.6 vs. 8.6 hours, p<0.001). Postoperatively, there was significantly increased red blood cell (RBC) transfusion (6.37 units vs. 4.47 units, p=0.007) and grade III and IV complications (57.3% vs. 40.6%, p=0.004). No difference was noted in ICU stay, total length of stay, hospital death and return to OT. In terms of respiratory complications, an increased incidence of pneumothorax (16.5% vs. 6.2%, p<0.001) was noted whilst pleural effusions and pneumonia occurrences were non-significant. Overall survival, revealed bilateral interventions in low-grade appendiceal mucinous neoplasm conferred an increased relative risk (p=0.037, RR=2.230, 95%CI=1.052-4.730). They did not have an effect on OS in colorectal cancer and mesothelioma.
CONCLUSION: Despite the increase in short-term morbidity, bilateral diaphragm interventions resulted in similar long-term survival to unilateral interventions.
Colorectal (Bowel) Cancer
Evaluation of appendiceal mucinous neoplasms with a new classification system and literature review.
Turk J Gastroenterol. 2018; 29(5):533-542 [PubMed] Article available free on PMC after 01/01/2020 Related Publications
Long-term outcomes in pediatric appendiceal carcinoids: Turkey experience.
Eur J Pediatr. 2018; 177(12):1845-1850 [PubMed] Related Publications
Goblet cell carcinoid of the appendix - diagnostic challenges and treatment updates: a case report and review of the literature.
J Med Case Rep. 2018; 12(1):275 [PubMed] Article available free on PMC after 01/01/2020 Related Publications
CASE PRESENTATION: We present the case of a 77-year-old Caucasian man with a history of stage I adenocarcinoma of transverse colon status post transverse colectomy who was incidentally found on surveillance colonoscopy to have an abnormal appendiceal orifice lesion. A biopsy revealed an appendiceal goblet cell carcinoid and he underwent a right hemicolectomy which revealed a pathologic stage III GCC for which he received eight cycles of adjuvant chemotherapy with capecitabine.
CONCLUSIONS: It is essential that patients who have tumors > 2 cm, are pT3 or pT4, have higher grade histology with signet ring (Tang grade B or grade C), locally advanced, or with positive surgical margins on appendectomy undergo a right hemicolectomy. Although there is no category 1 evidence, consensus recommendations are that patients with stage II (particularly Tang B and C) and stage III GCC be offered adjuvant chemotherapy with a regimen based on 5-fluorouracil, as these patients are known to have high rates of relapse.
