Chondrosarcoma
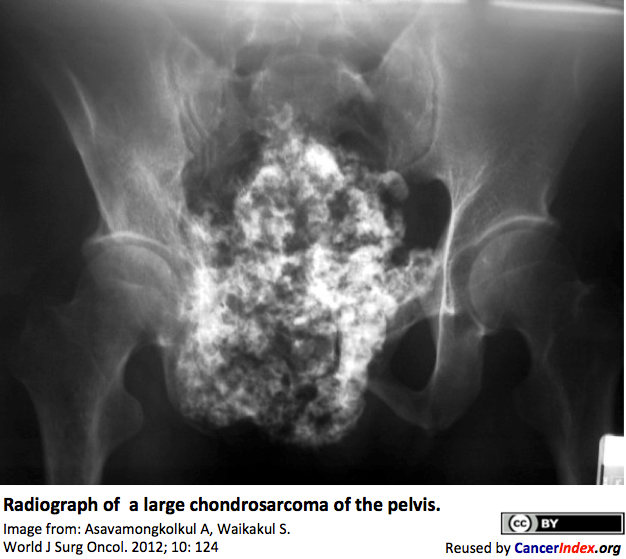 Chondrosarcoma is a type of cancer that forms in bone cartilage. The most frequent primary sites are the pelvis, shoulder, ribs, or at the ends of the arms and legs. Chondrosarcoma can occur at any age but is more common in people older than 40 years.
Chondrosarcoma is a type of cancer that forms in bone cartilage. The most frequent primary sites are the pelvis, shoulder, ribs, or at the ends of the arms and legs. Chondrosarcoma can occur at any age but is more common in people older than 40 years.
 Information for Patients and the Public Information for Health Professionals / Researchers Latest Research Publications
Information for Patients and the Public Information for Health Professionals / Researchers Latest Research Publications Mesenchymal Chondrosarcoma Bone Cancer Resources Molecular Genetics of Chondrosarcoma
Mesenchymal Chondrosarcoma Bone Cancer Resources Molecular Genetics of ChondrosarcomaInformation Patients and the Public (3 links)

Macmillan Cancer Support![]() Content is developed by a team of information development nurses and content editors, and reviewed by health professionals. Further info.
Content is developed by a team of information development nurses and content editors, and reviewed by health professionals. Further info.
Liddy Shriver Sarcoma Initiative
The site includes an overview of Chondrosarcoma, more detailed information, support and research.
 Chondrosarcoma Support Group - Online Forum
Chondrosarcoma Support Group - Online Forum
A moderated forum for patients and carers set-up by a patient.
Information for Health Professionals / Researchers (4 links)
- PubMed search for publications about Chondrosarcoma - Limit search to: [Reviews]
PubMed Central search for free-access publications about Chondrosarcoma
MeSH term: Chondrosarcoma US National Library of Medicine PubMed has over 22 million citations for biomedical literature from MEDLINE, life science journals, and online books. Constantly updated.
PubMed has over 22 million citations for biomedical literature from MEDLINE, life science journals, and online books. Constantly updated.
BoneTumour.org
Detailed overview with numerous radiology and histopathology images. Covers Incidence and Demographics, symptoms and presentation, differential diagnosis, histopathology, and prognosis.
Medscape
A detailed referenced article by Dr Palaniappan Lakshmanan and colleagues, including radiology and histology images.
 Chondrosarcoma - Foot and Ankle
Chondrosarcoma - Foot and Ankle
BoneTumour.org
Detailed overview with numerous radiology and pathology images.
Latest Research Publications
This list of publications is regularly updated (Source: PubMed).
Comparative analysis of the levels of soluble forms of receptor and ligand of the immunity control point PD-1/PD-L1 in the blood serum of patients with typical bone osteosarcoma and chondrosarcoma.
Klin Lab Diagn. 2020; 65(11):669-675 [PubMed] Related Publications
Development and external validation of nomograms to predict sarcoma-specific death and disease progression after surgical resection of localized high-grade conventional primary central chondrosarcoma and dedifferentiated chondrosarcoma.
Bone Joint J. 2020; 102-B(12):1752-1759 [PubMed] Related Publications
METHODS: The study population consisted of 391 patients from two international sarcoma centres (development cohort) who had undergone definitive surgery for a localized high-grade (histological grade II or III) conventional primary central chondrosarcoma or dedifferentiated chondrosarcoma. Disease progression captured the first event of either metastasis or local recurrence. An independent cohort of 221 patients from three additional hospitals was used for external validation. Two nomograms were internally and externally validated for discrimination (c-index) and calibration plot.
RESULTS: In the development cohort, the CISSD at ten years was 32.9% (95% confidence interval (CI) 19.8% to 38.4%). Age at diagnosis, grade, and surgical margin were found to have significant effects on CISSD and CIDP in multivariate analyses. Maximum tumour diameter was also significantly associated with CISSD. In the development cohort, the c-indices for CISSD and CIDP at five years were 0.743 (95% CI 0.700 to 0.819) and 0.761 (95% CI 0.713 to 0.800), respectively. When applied to the validation cohort, the c-indices for CISSD and CIDP at five years were 0.839 (95% CI 0.763 to 0.916) and 0.749 (95% CI 0.672 to 0.825), respectively. The calibration plots for these two nomograms demonstrated good fit.
CONCLUSION: Our nomograms performed well on internal and external validation and can be used to predict CISSD and CIDP after resection of localized high-grade conventional primary central and dedifferentiated chondrosarcomas. They provide a new tool with which clinicians can assess and advise individual patients about their prognosis. Cite this article:
 Bone Cancers
Bone Cancers
Unresectable Chondrosarcomas Treated With Carbon Ion Radiotherapy: Relationship Between Dose-averaged Linear Energy Transfer and Local Recurrence.
Anticancer Res. 2020; 40(11):6429-6435 [PubMed] Related Publications
PATIENTS AND METHODS: Thirty patients treated with CIRT for grade 2 chondrosarcoma were included. Dose-averaged LET (LET
RESULTS: The mean LET
CONCLUSION: LET
Comparison of reconstructive techniques following oncologic intraarticular resection of proximal humerus.
J Surg Oncol. 2021; 123(1):133-140 [PubMed] Related Publications
METHODS: A total of 83 (42 females, 41 males) patients undergoing an intraarticular resection of the humerus were reviewed. Reconstructions included 30 reverse and 53 hemiarthroplasty; including hemiarthroplasty EPR (n = 36) and APC (n = 17), and reverse EPR (n = 20) and APC (n = 10).
RESULTS: Reverse reconstructions had improved forward elevation (85° vs. 44°, p < .001) and external rotation (30° vs. 21°; p < .001) versus a hemiarthroplasty. Reverse reconstructions had improved American Shoulder and Elbow Surgeons scores (65 vs. 57; p = .01) and Musculoskeletal Tumor Society 93 scores (72 vs. 63; p < .001) versus hemiarthroplasty. Subluxation of the reconstruction was a common (n = 23, 27%), only occurring in hemiarthroplasty patients (EPR [n = 13, 36%] and APC [n = 10, 59%]).
CONCLUSION: The current series highlights the improved functional outcome in patients undergoing reconstruction with a reverse arthroplasty compared to the traditional hemiarthroplasty. Currently reverse shoulder arthroplasty (APC or EPR) is our preferred methods of reconstruction in this patient population.
Bone Cancers
A system-level approach identifies HIF-2α as a critical regulator of chondrosarcoma progression.
Nat Commun. 2020; 11(1):5023 [PubMed] Free Access to Full Article Related Publications
Utility of Bone Scintigraphy and PET-CT in the Surgical Staging of Skeletal Chondrosarcoma.
Anticancer Res. 2020; 40(10):5735-5738 [PubMed] Related Publications
PATIENTS AND METHODS: We reviewed 138 (87 males, 51 female) patients, mean age 54±20 years, with a chondrosarcoma, who had completed a bone scintigraphy or PET/CT as part of surgical staging. Sensitivity, specificity, and positive/negative predictive value of the scans was calculated.
RESULTS: Seventeen (12%) patients had a positive bone scintigraphy or PET-CT for skeletal metastases. In cases of bone scintigraphy (n=11), 6 were benign and 5 were skeletal metastases. In cases of PET-CT, 6 were skeletal metastases, 3 were positive and 3 benign. All positive cases regarded dedifferentiated chondrosarcoma. The overall sensitivity and specificity of a bone scan or PET-CT was 100% and 93.1%; with a positive and negative predictive value of 47.1% and 100%, respectively.
CONCLUSION: Skeletal metastases at presentation of chondrosarcoma are rare and associated with dedifferentiated chondrosarcoma. Bone scintigraphy or PET-CT should only be performed in cases of high grade and dedifferentiated histology.
Promotion of Chondrosarcoma Cell Survival, Migration and Lymphangiogenesis by Periostin.
Anticancer Res. 2020; 40(10):5463-5469 [PubMed] Related Publications
MATERIALS AND METHODS: To evaluate the effect of periostin on the proliferation of chondrosarcoma cells, MTT assay was performed on SW1353 cells and periostin knockdown SW1353 cells. Migration activity was examined using Boyden chamber.
RESULTS: Periostin, secreted from chondrosarcoma cells, was found to support proliferation, and maintain stemness and migration of chondrosarcoma cells. Periostin also induced proliferation and migration of lymphatic endothelial cells.
CONCLUSION: Periostin plays an important role in chondrosarcoma development and disease progression.
Angiogenesis and Cancer
Diagnoses, treatment, and oncologic outcomes in patients with calcaneal malignances: Case series, systematic literature review, and pooled cohort analysis.
J Surg Oncol. 2020; 122(8):1731-1746 [PubMed] Related Publications
AIMS: (1) describe the demographics of calcaneal malignancies in a large cohort; (2) describe survival after amputation versus limb-salvage surgery for high-grade tumors.
METHODS: Study group: a "pooled" cohort of patients with primary calcaneal malignancies treated at two cancer centers (1984-2015) and systematic literature review. Kaplan-Meier analyses described survival across treatment and diagnostic groups; proportional hazards modeling assessed mortality after amputation versus limb salvage.
RESULTS: A total of 131 patients (11 treated at our centers and 120 patients from 53 published studies) with a median 36-month follow-up were included. Diagnoses included Ewing sarcoma (41%), osteosarcoma (30%), and chondrosarcoma (17%); 5-year survival rates were 43%, 73% (70%, high grade only), and 84% (60%, high grade only), respectively. Treatment involved amputation in 52%, limb salvage in 27%, and no surgery in 21%. There was no difference in mortality following limb salvage surgery (vs. amputation) for high-grade tumors (HR 0.38; 95% CI 0.14-1.05), after adjusting for Ewing sarcoma diagnosis (HR 5.15; 95% CI 1.55-17.14), metastatic disease at diagnosis (HR 3.88; 95% CI 1.29-11.64), and age (per-year HR 1.04; 95% CI 1.02-1.07).
CONCLUSIONS: Limb salvage is oncologically-feasible for calcaneal malignancies.
Translocase of the outer mitochondrial membrane complex subunit 20 (TOMM20) facilitates cancer aggressiveness and therapeutic resistance in chondrosarcoma.
Biochim Biophys Acta Mol Basis Dis. 2020; 1866(12):165962 [PubMed] Article available free on PMC after 01/12/2021 Related Publications
Apoptosis Bone Cancers
Economics of the Management of Craniospinal Chordoma and Chondrosarcoma and the feasibility of the bundled payment model.
BMC Neurol. 2020; 20(1):312 [PubMed] Article available free on PMC after 01/12/2021 Related Publications
METHODS: We selected patients with chordoma/chondrosarcoma from inpatient admission table using the International Classification of Disease, 9th (ICD-9), and 10th (ICD-10) revision codes. We collected the patients' demographics and insurance type at the index hospitalization. We recorded the following outcomes length of stay, total payment, discharge disposition, and complications for the index hospitalization. For post-discharge, we collected the 30 days and 3/6/12 months inpatient admission, outpatient service, and medication refills. Continuous variables were summarized by means with standard deviations, median with interquartile and full ranges (minimum-maximum); Continuous outcomes were compared by nonparametric Wilcoxson rank-sum test. All tests were 2-sided with a significance level of 0.05. Statistical data analysis was performed in SAS 9.4 (SAS Institute, Inc, Cary, NC).
RESULTS: The population size was 2041 patients which included 1412 patients with cranial (group1), 343 patients with a mobile spine (group 2), and 286 patients with sacrococcygeal (group 3) chordoma and chondrosarcoma. For index hospitalization, the median length of stay (days) was 4, 6, and 7 for groups 1, 2, and 3 respectively (P<.001). The mean payments were ($58,130), ($84,854), and ($82,440), for groups 1, 2, and 3 respectively (P=.02). The complication rates were 30%, 35%, and 43% for groups 1, 2, and 3 respectively (P<.001). Twelve months post-discharge, the hospital readmission rates were 44%, 53%, and 65% for groups 1, 2, and 3, respectively (P<.001). The median payments for this period were ($72,294), ($76,827), and ($101,474), for groups 1, 2, and 3, respectively (P <.001).
CONCLUSION: The management of craniospinal chordoma and chondrosarcoma is costly and may extend over a prolonged period. The success of BPCI requires a joint effort between insurers and hospitals. Also, it should consider patients' comorbidities, the complexity of the disease. Finally, the adoptionof quality improvement programs by hospitals can help with cost reduction.
USA
Extraskeletal myxoid chondrosarcoma: A high incidence of metastatic disease to lymph nodes.
J Surg Oncol. 2020; 122(8):1662-1667 [PubMed] Related Publications
METHODS: Thirty (21 males, 9 females) patients, mean age 50 ± 16 years, with ESMC were reviewed. The tumors were most commonly located in the lower extremity (n = 23, 77%) and the mean tumor size and volume were 9 ± 5 cm and 490 ± 833 cm
RESULTS: Six (20%) patients either presented (n = 3, 10%) or developed (n = 3, 10%) lymph node metastatic disease. When comparing patients without, with lymph node metastasis and metastasis elsewhere, patients with lymph nodes metastasis had worse survival than those without metastasis, however better 10-year disease specific survival than those with metastasis elsewhere (100% vs 62% vs 0%; P < .001).
CONCLUSION: There is a high incidence of lymph node metastatic disease in patients with ESMC. Although survival in these patients is worse compared to those without metastasis, their survival is better than those with metastasis elsewhere. Due to the high incidence of lymph node metastatic disease, preoperative staging of the lymph node should be considered.
The nose lid for the endoscopic endonasal procedures during COVID-19 era: technical note.
Acta Neurochir (Wien). 2020; 162(10):2335-2339 [PubMed] Article available free on PMC after 01/12/2021 Related Publications
METHOD: Our department, according to the actual COVID-19 protocol national guidelines, has suspended elective procedures and, in the last month, only three patients underwent to endoscopic endonasal procedures, due to urgent conditions (a pituitary apoplexy, a chondrosarcoma causing cavernous sinus syndrome, and a pituitary macroadenoma determining chiasm compression). We describe peculiar surgical technique modifications and the use of an endonasal face mask, i.e., the nose lid, to be applied to the patient during transnasal procedures for skull base pathologies as a further possible COVID-19 mitigation strategy.
RESULTS: The nose lid is cheap, promptly available, and can be easily assembled with the use of few tools available in the OR; this mask allows to both operating surgeon and his assistant to perform wider surgical maneuvers throughout the slits, without ripping it, while limiting the nostril airflow.
CONCLUSIONS: Transnasal surgery, transgressing respiratory mucosa, can definitely increase the risk of virus transmission: we find that adopting further precautions, above all limiting high-speed drill can help preventing or at least reducing aerosol/droplets. The creation of a non-rigid face mask, i.e., the nose lid, allows the comfortable introduction of instruments through one or both nostrils and, at the same time, minimizes the release of droplets from the patient's nasal cavity.
Pituitary Tumors
Inhibition of Autograft Bone Resorption by Antibone Resorptive Agents After Spinal Reconstruction Surgery for Extensive Cervical Chondrosarcoma: A Case Report with a 10-Year Follow-Up.
World Neurosurg. 2020; 142:239-245 [PubMed] Related Publications
CASE DESCRIPTION: A 42-year-old Asian woman presented with neck pain, tumorous masses on the neck, and left arm pain. Magnetic resonance imaging and computed tomography of the cervical spine showed extensive malignant spinal tumor. Histological examination of tumor biopsy revealed grade I chondrosarcoma. Complete resection of the tumor was performed using an anterior-posterior approach, followed by anterior iliac bone grafting and posterior spinal instrumentation. No tumor recurrence was observed on magnetic resonance imaging at final follow-up after 10 years. However, grafted bone resorption was identified immediately after surgery due to stress shielding by robust spinal instrumentation. To inhibit resorption of grafted bone, the bisphosphonate minodronate was administered for 5 years from 3 years postoperatively, before being replaced by denosumab from 8 years postoperatively. After use of these antibone resorptive agents, grafted bone resorption stopped.
CONCLUSIONS: Anteriorly grafted bone resorption due to stress shielding may occur after reconstructive cervical spine surgery with robust posterior spinal instrumentation. Bisphosphonates and denosumab may be considered to inhibit grafted bone resorption.
Bisphosphonates
Intra-articular Extraskeletal EWSR1-Negative NR4A3-Positive Myxoid Chondrosarcoma: A Case Report.
JBJS Case Connect. 2020 Apr-Jun; 10(2):e0614 [PubMed] Related Publications
CONCLUSION: This is a unique case of intra-articular EMC of the knee with a rare molecular fingerprint and an unusually positive outcome.
Quantitative SPECT/CT for differentiating between enchondroma and grade I chondrosarcoma.
Sci Rep. 2020; 10(1):10587 [PubMed] Article available free on PMC after 01/12/2021 Related Publications
Diagnostic role of neutrophil-to-lymphocyte ratio and monocyte-to-lymphocyte ratio in patients with enchondroma and low-grade chondrosarcoma.
Jt Dis Relat Surg. 2020; 31(2):286-290 [PubMed] Article available free on PMC after 01/12/2021 Related Publications
PATIENTS AND METHODS: One-hundred-and-one patients (44 males, 57 females; mean age 53.6±11.5 years; range, 21 to 85 years) diagnosed with enchondroma and low-grade chondrosarcoma in Ankara Oncology Training and Research Hospital between January 2010 and December 2019 were included in this retrospective study. Patients' age, gender, location and type of tumor, and pre-treatment complete blood count results were acquired. One-hundred patients (48 males, 52 females; mean age 50.9±13.6 years; range, 19 to 76 years) with complete blood count results admitted to the same center for reasons other than fracture, infection or tumors with similar age and gender to the aforementioned study group were included as healthy controls.
RESULTS: Neutrophil-to-lymphocyte ratio and MLR of the study group were found to be significantly higher than the control group (p<0.001). Neutrophil-to-lymphocyte ratio and MLR held diagnostic importance with statistically significant cut-off values. Statistically significant cut-offs for NLR and MLR were ≥2.0 (sensitivity=73.3%, specificity=67%) and ≥0.2 (sensitivity=76.2%, specificity=63%), respectively. Multivariate logistic regression analysis was performed adjusting for age and gender and NLR ≥2 [odds ratio (OR)=3.1] or MLR ≥0.2 (OR=2.9) were found to be associated with approximately three-fold risk for diagnosis of enchondroma or low-grade chondrosarcoma.
CONCLUSION: The NLR and MLR have diagnostic value in cartilaginous tumors such as enchondroma and low-grade chondrosarcoma. However, our results do not support utilization of NLR and MLR as diagnostic value for differentiation of enchondroma and low-grade chondrosarcoma.
Bone Cancers
Evaluation of factors affecting survival rate in primary bone sarcomas with extremity and pelvis involvement.
Acta Orthop Traumatol Turc. 2020; 54(3):234-244 [PubMed] Article available free on PMC after 01/12/2021 Related Publications
METHODS: A total of 114 patients (64 male and 50 female) with osteosarcoma, chondrosarcoma, or Ewing's sarcoma treated between 2005 and 2013 were included in this study. All the patients received standard treatment and were followed up regularly. In all, 44 cases of (conventional and telangiectatic) osteosarcoma, 30 cases of Ewing's sarcoma, and 40 cases of high-grade chondrosarcoma were identified using the Bone and Soft Tissue Tumor Registry. Gender, age, tumor size and localization, pathological fractures, histopathological type, grade, surgical treatment, adjuvant treatments, relapse of the disease, and postoperative complication data were obtained from follow-up forms. The learning curve of institutional expertise was also evaluated. The patient survival rate was calculated using the Kaplan-Meier method, and log-rank statistical methods were used to compare survival rates.
RESULTS: The mean length of survival of the patients was 72 months. There was a 56% 5-year survival rate, and the event-free survival rate was 53%. The survival of patients with Ewing's sarcoma whose prodromal period was less than 12 weeks was significantly higher than that of the other groups (p=0.031). The survival of patients with tumor size greater than 150 cc, with local recurrence and distant metastases was low for all groups. Survival rates were significantly lower in osteosarcoma and Ewing's sarcoma patients with stage III tumor or metastasis at diagnosis. The survival of patients with osteosarcoma diagnosed between 2010 and 2013 was significantly higher than that of the earlier group (p=0.02).
CONCLUSION: Decreasing the prodromal period (early diagnosis) can improve survival by preventing the local and systemic spread of the tumor. Increase in the surgical experience is likely to have a positive effect on survival rates, especially for patients with osteosarcoma. The relapse of the disease is a poor prognostic factor for survival despite aggressive surgery and adjuvant therapies.
LEVEL OF EVIDENCE: Level IV, Therapeutic study.
MRI radiomics-based machine-learning classification of bone chondrosarcoma.
Eur J Radiol. 2020; 128:109043 [PubMed] Related Publications
METHODS: We retrospectively enrolled 58 patients with histologically-proven low-grade/atypical cartilaginous tumor of the appendicular skeleton (n = 26) or higher-grade chondrosarcoma (n = 32, including 16 appendicular and 16 axial lesions). They were randomly divided into training (n = 42) and test (n = 16) groups for model tuning and testing, respectively. All tumors were manually segmented on T1-weighted and T2-weighted images by drawing bidimensional regions of interest, which were used for first order and texture feature extraction. A Random Forest wrapper was employed for feature selection. The resulting dataset was used to train a locally weighted ensemble classifier (AdaboostM1). Its performance was assessed via 10-fold cross-validation on the training data and then on the previously unseen test set. Thereafter, an experienced musculoskeletal radiologist blinded to histological and radiomic data qualitatively evaluated the cartilaginous tumors in the test group.
RESULTS: After feature selection, the dataset was reduced to 4 features extracted from T1-weighted images. AdaboostM1 correctly classified 85.7 % and 75 % of the lesions in the training and test groups, respectively. The corresponding areas under the receiver operating characteristic curve were 0.85 and 0.78. The radiologist correctly graded 81.3 % of the lesions. There was no significant difference in performance between the radiologist and machine learning classifier (P = 0.453).
CONCLUSIONS: Our machine learning approach showed good diagnostic performance for classification of low-to-high grade cartilaginous bone tumors and could prove a valuable aid in preoperative tumor characterization.
Bone Cancers
Can MRI differentiate between atypical cartilaginous tumors and high-grade chondrosarcoma? A systematic review.
Acta Orthop. 2020; 91(4):471-478 [PubMed] Related Publications
Bone Cancers
Insulin-Like Growth Factor 1 (IGF1) Pathway Member Polymorphisms Are Associated with Risk and Prognosis of Chondrosarcoma.
Med Sci Monit. 2020; 26:e923853 [PubMed] Article available free on PMC after 01/12/2021 Related Publications
Leucine and branched-chain amino acid metabolism contribute to the growth of bone sarcomas by regulating AMPK and mTORC1 signaling.
Biochem J. 2020; 477(9):1579-1599 [PubMed] Related Publications
Reconstruction of forearm support with ulnar translocation after resection of chondrosarcoma in the proximal radius.
Orthopade. 2020; 49(11):1006-1012 [PubMed] Related Publications
Bone Cancers
Cold Atmospheric Plasma Treatment of Chondrosarcoma Cells Affects Proliferation and Cell Membrane Permeability.
Int J Mol Sci. 2020; 21(7) [PubMed] Article available free on PMC after 01/12/2021 Related Publications
Proximal Femur Chondrosarcoma Misdiagnosed as Hip Arthritis: A Case Report.
JBJS Case Connect. 2020 Jan-Mar; 10(1):e0324 [PubMed] Related Publications
CONCLUSIONS: Chondrosarcoma does not always present with a classical clinical picture or imaging, and it can be misdiagnosed. Practitioners should be highly suspicious of malignant disease as a cause for hip pain even if there is no direct indication of a neoplasm such as chondrosarcoma.
Phase I Study of the Mutant IDH1 Inhibitor Ivosidenib: Safety and Clinical Activity in Patients With Advanced Chondrosarcoma.
J Clin Oncol. 2020; 38(15):1693-1701 [PubMed] Article available free on PMC after 20/05/2021 Related Publications
PATIENTS AND METHODS: This phase I multicenter open-label dose-escalation and expansion study of ivosidenib monotherapy enrolled patients with mutant
RESULTS: Twenty-one patients (escalation, n = 12; expansion, n = 9) with advanced chondrosarcoma received ivosidenib (women, n = 8; median age, 55 years; range, 30-88 years; 11 had received prior systemic therapy). Treatment-emergent adverse events (AEs) were mostly grade 1 or 2. Twelve patients experienced grade ≥ 3 AEs; only one event was judged treatment related (hypophosphatemia, n = 1). Plasma 2-HG levels decreased substantially in all patients (range, 14%-94.2%), to levels seen in healthy individuals. Median progression-free survival (PFS) was 5.6 months (95% CI, 1.9 to 7.4 months); the PFS rate at 6 months was 39.5%. Eleven (52%) of 21 patients experienced stable disease.
CONCLUSION: In patients with chondrosarcoma, ivosidenib showed minimal toxicity, substantial 2-HG reduction, and durable disease control. Future studies of ivosidenib monotherapy or rational combination approaches should be considered in patients with advanced mutant
Conditional Survival Analysis for Spinal Chondrosarcoma Patients After Surgical Resection.
Spine (Phila Pa 1976). 2020; 45(16):1110-1117 [PubMed] Related Publications
OBJECTIVE: To evaluate conditional survival after surgical resection for spinal chondrosarcoma patients.
SUMMARY OF BACKGROUND DATA: Survival estimates are usually reported as survival from the time of surgery, but survival probabilities can change over time. Conditional survival, which is a measure of prognosis for patients who have survived a defined period of time, may be more clinically precise and relevant. However, data on conditional survival for spinal chondrosarcoma patients after surgical resection are still lacking.
METHODS: We used the Surveillance, Epidemiology, and End Results (SEER) database to identify 436 spinal chondrosarcoma patients who underwent surgical resection from 1994 and 2013. Kaplan-Meier analyses and Cox regression modeling were performed to evaluate prognostic factors associated with overall survival. Five-year conditional survival (i.e., probability of surviving an additional 5 years, given that a patient has already survived x years) was calculated as 5-CS(x) = OS(x+5)/OS(x). The effect of prognostic factors on conditional survival was also explored.
RESULTS: Four hundred thirty six patients were included in the study cohort. Overall, 1-, 3-, and 5-year overall survival were 92.8%, 79.1%, and 70.3%, respectively. Five-year conditional survival at 1, 3, and 5 years after surgery were 72.9%, 79.0%, and 87.5%. The overall survival rates were lower in cases of age more than or equal to 60 years, male patient, dedifferentiated subtype, Grade III tumor, tumor size more than or equal to 10 cm, distant metastasis, and radiotherapy. Conditional survival improved over time in each subgroup divided by age, sex, race, year of diagnosis, grade, tumor size, extent of disease (EOD), and radiotherapy. In addition, patients with the least favorable prognosis at baseline experienced the greatest increase in 5-year conditional survival over time (e.g., Grade I/II: 78.0%-89.7%, Δ11.7% vs. Grade III: 36.5%-66.6%, Δ30.1%; Localized/Regional: 72.9%-88.1%, Δ15.2% vs. Distant: 43.5%-74.1%, Δ30.6%).
CONCLUSION: Conditional survival for spinal chondrosarcoma patients after surgical resection improves over time, especially for patients with initial high-risk characteristics. Information derived from conditional survival analysis may provide individualized approaches to surveillance and treatment of spinal chondrosarcoma.
LEVEL OF EVIDENCE: 4.
Bone Cancers
Therapeutic strategy for tracheal chondrosarcoma: report of two cases.
Monaldi Arch Chest Dis. 2020; 90(1) [PubMed] Related Publications
Tracheal (windpipe) Cancer
Natural history of Ollier disease and Maffucci syndrome: Patient survey and review of clinical literature.
Am J Med Genet A. 2020; 182(5):1093-1103 [PubMed] Related Publications
Ovarian Cancer
Risk stratification for central conventional chondrosarcoma of bone: A novel system predicting risk of metastasis and death in the Cancer Registry of Norway cohort.
J Surg Oncol. 2020; 121(7):1115-1125 [PubMed] Related Publications
METHOD: We selected 149 cases from the Cancer Registry of Norway. Cox proportional hazard models were estimated. Based on these results a dichotomous risk classification was proposed and presented by Kaplan-Meier estimates for rates of local recurrence, metastasis, and disease-specific survival.
RESULTS: The influence of axial skeletal location (Hazard ratio [HR] = 19.06), a soft tissue component ≥1 cm (HR = 13.45), and histological grade 3 (HR = 16.46) are all significant in predicting the rate of metastasis. The creation of a variable combining axial skeletal location and a soft tissue component ≥1 cm strongly predicts the risk of metastasis (HR = 14.02; P < .001) and death (HR = 2.74; P = .030) at multivariate analysis, making the histological grade insignificant. Together with metastasis at diagnosis (HR = 285.65; P < .001), this forms the basis of our proposed risk stratification, producing a small high-risk group (39 cases with 33% risk of metastasis) and a large low-risk group (103 cases with 2% risk of metastasis) without a histological grade.
CONCLUSION: Axial skeletal location and a soft tissue component ≥1 cm combined divides a CCCS cohort into low- and high-risk groups without a histological grade.
Bone Cancers
